
To the Editor,
New technologies have improved the effectiveness of treatments for cardiovascular diseases, yet these technologies pose poorly explored challenges. Therefore, a study was conducted in Spain to find out about the perspective of doctors and administrators on the implications of technology in the management of coronary artery disease and peripheral arterial disease.
The insights and perspectives of doctors and administrators were obtained using the Delphi method following the RAND/UCLA Appropriateness Method (RUAM).1 A scientific committee including 6 cardiologists, 1 vascular surgeon, and 1 interventional radiologist selected the panel of doctors (16 cardiologists, 3 endocrinologists, 3 vascular surgeons, 1 internist, and 1 surgeon specialized in diabetic foot disease), and administrators (12 administrators from both the public and private sectors) (annex 1 of the supplementary data). The doctors’ questionnaire had 112 items and the administrators’ one 79 (74 items were common to both panels). The panellists scored the relevance of each item on a scale from 1 (irrelevant) to 9 (maximum relevance). «Agreement» was defined as less than a third of the panelists giving scores from 1 to 3 to a given item, and less than a third gave scores from 7 to 9. «Low relevance» items were those whose median scores were < 4, «high relevance» items with median scores ≥ 7, and «medium relevance» items with median scores ≥ 4 and < 7.1 Concordance between doctors and administrators in the 74 items studied was measured using the kappa index (κ).2 Figure 1 shows the study diagram.
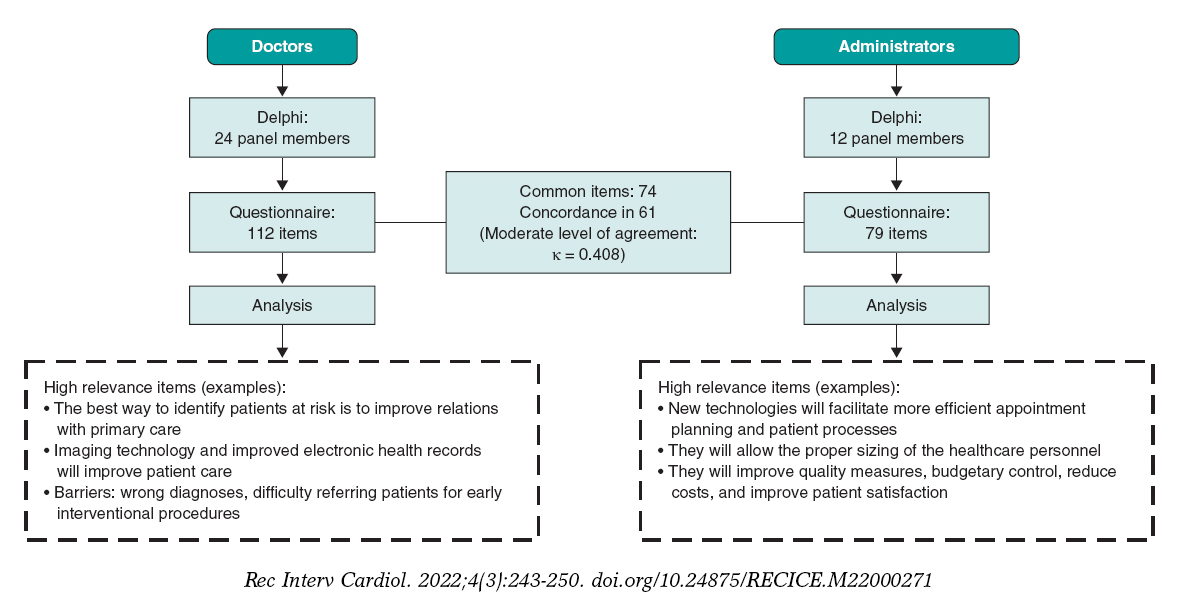
Figure 1. Summary of the study diagram.
Some of the «high relevance» items scored by doctors and administrators had to do with technology improving patient care, the identification of risk factors, the ability to treat patients from the start with the corresponding reduction of readmissions and costs, and with the ability to achieve more accurate diagnoses. Doctors believe that the best measure to identify patients at risk is to improve relations with primary care. Reduced time spent with each patient, the scarcity of resources to make patients change their lifestyles, and the lack of facilities available for rehabilitation purposes are significant limitations for doctors. Doctors and administrators believe that within the next few years better solutions will come along for the diagnosis and treatment of cardiovascular diseases. However, some of the barriers they refer to are the difficulties referring patients for early interventional procedures or the scarcity of personnel for the early management of patients (tables 1-23 of the supplementary data).
Compared to administrators, doctors insist that technology requires training, which requires time they don’t have (figure 2A). Administrators, however, insist that technology allows the proper sizing of the healthcare personnel (figure 2B; tables 24-32 of the supplementary data). The differences found are indicative of a moderate level of agreement between doctors and administrators (κ = 0.408)2 (table 1).
Table 1. Concordance in the category of relevance between the panel of doctors and the panel of administrators
| Panel of administrators | ||||||
|---|---|---|---|---|---|---|
| Number of items scored with relevance | ||||||
| Relevance | High | Medium | Low | Overall | ||
| Panel of doctors | Number of items scored with relevance | High | 56 | 5 | 0 | 61 |
| Medium | 5 | 5 | 3 | 13 | ||
| Low | 0 | 0 | 0 | 0 | ||
| Overall | 61 | 10 | 3 | 74 | ||
|
κ index, 0.408 (moderate level of agreement). |
||||||
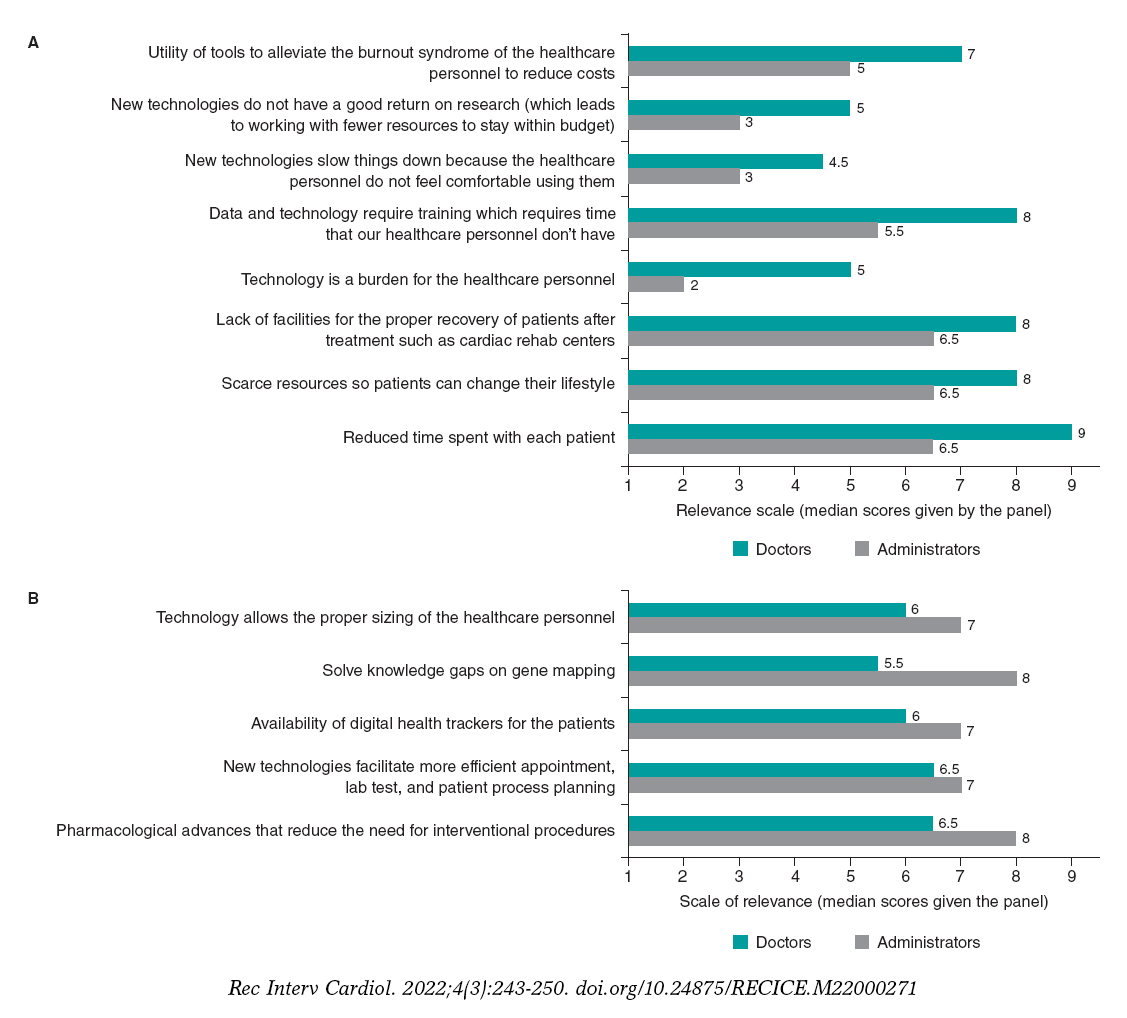
Figura 2. A: ítems puntuados con mayor categoría de relevancia por los médicos frente a los administradores. B: ítems puntuados con mayor categoría de relevancia por los administradores frente a los médicos.
These findings suggest that both doctors and administrators believe that technological advances have improved patient care. However, they also identify certain barriers. The moderate level of agreement between doctors and administrators is understandable, but the success of each center largely depends on this level of agreement between the two. For these reasons, different strategies have been proposed for doctors and administrators to come closer in a coherent and collaborative way.3
These strategies and those aimed at eliminating the barriers and limitations found are particularly relevant in interventional cardiology. Recommendations on requirements and equipment in interventional cardiology recently published in Spain are some of these strategies.4 These recommendations establish the structural and functional requirements of each center regarding human resources, training, competences, and material resources. Also, they develop the model of satellite or supervised cath labs as an efficient alternative for lower level hospitals.4 The implementation of these strategies can improve the quality, efficiency, and equal access to interventional cardiology in Spain.
Evidence on the validity and reproducibility of the Delphi format used in our study (RUAM)5 plus the fact that it is the method used to develop appropriate use criteria for coronary revascularization6 suggests that the findings of this study represent reasonably well the perspectives of doctors and administrators on the implications of technology in the management of cardiovascular diseases, and specifically interventional cardiology in Spain.
FUNDING
This study was funded by Abbott Vascular that did not participate in the design of the study or in the processes of data mining, handling, analysis or interpretation.
AUTHORS’ CONTRIBUTIONS
All authors contributed to the drafting of this manuscript.
CONFLICTS OF INTEREST
None whatsoever.
ACKNOWLEDGEMENTS
The authors wish to thank Dr. Vicente Mainar (cardiologist at Hospital General de Alicante), Dr. Mariano de Blas Bravo (interventional radiologist at Hospital Donostia, San Sebastián), and Dr. José M. de la Torre Hernández (cardiologist at Hospital Marqués de Valdecilla, Santander) who, together with the authors, were involved this project scientific committee, and appointed the panellists who became members of the panel of medical experts and administrators.
Also, the authors wish to thank the members from the panels of expert doctors and administrators for their kind participation in the Delphi method, and collaboration in the study since their answers to the questionnaires allowed us to conduct this project. The list of members from each panel of experts is shown in annex 2 of the supplementary data.
SUPPLEMENTARY DATA

REFERENCES
1. Fitch K, Bernstein SJ, Aguilar MD, Burnand B, LaCalle JR. The RAND/UCLA appropriateness method user's manual. Rand Corp Santa Monica CA. MR-1269. 2001.
2. McGinn T, Wyer PC, Newman TB, et al. Tips for learners of evidencebased medicine:3. Measures of observer variability (kappa statistic). CMAJ. 2004;171:1369-1373.
3. Bhardwaj A. Alignment between physicians and hospital administrators:historical perspective and future directions. Hosp Pract. 2017;45:81-87.
4. Moreno R, Ojeda S, Romaguera R, et al. Actualización de las recomendaciones sobre requisitos y equipamiento en cardiología intervencionista. REC Interv Cardiol. 2021;3:33-44.
5. Lawson EH, Gibbons MM, Ko CY, Shekelle PG. The appropriateness method has acceptable reliability and validity for assessing overuse and underuse of surgical procedures. J Clin Epidemiol. 2012;65:1133-1143.
6. Patel MR, Calhoon JH, Dehmer GJ, et al. CC/AATS/AHA/ASE/ASNC/SCAI/SCCT/STS 2017 Appropriate Use Criteria for Coronary Revascularization in Patients With Stable Ischemic Heart Disease. J Am Coll Cardiol. 2017;69:2212-2241.












