
Abstract
Introduction and objectives: Accessing sharply angulated side branches using intracoronary guidewires sometimes poses great challenges, and even after using its distal end for accessing purposes, it usually prolapses inside the main vessel. We hereby present an easy way to perform these procedures using a specific guidewire for the management of chronic total occlusions.
Methods: From January 2017 through September 2018, patients with lesions on sharply angulated side or large branches that required protection in bifurcations were approached using straight, angled tip and/or double-lumen microcatheters with regular guidewires. In cases of unsuccessful access, a specific wire designed for chronic total occlusions was used with the straight tip microcatheter after a drastic overhaul of the shape in its distal end.
Results: In 9 patients access to the side branch was not achieved with the initial strategy, in 3 patients due to access inability and in the remaining 6 due to guidewire prolapse when trying to advance the microcatheter. In all 9 cases, the access could be completed using the Gaia First guidewire that combines an excellent torque with enough rigidity to prevent the prolapse of the tip. All procedures were performed without complications.
Conclusions: The percutaneous coronary intervention of sharply angulated side branches can be challenging when advancing the guidewire. However, these procedures can be performed easily and quickly with a specific guidewire for the managemenf of chronic total occlusions.
Keywords: Bifurcation. Coronary guidewire. Angulated lesion. Chronic total occlusion.
Resumen
Introducción y objetivos: El acceso con la guía intracoronaria a las ramas laterales con origen muy angulado en ocasiones presenta gran dificultad, e incluso después de acceder con el extremo distal frecuentemente se produce su prolapso en el vaso principal. Presentamos una forma fácil de realizar estos procedimientos con el uso de una guía específica de oclusión crónica.
Métodos: Entre enero de 2017 y septiembre de 2018, los pacientes con lesiones en las ramas laterales o en ramas de gran tamaño que requerían protección en las bifurcaciones cuyo origen era muy angulado se abordaron con microcatéteres recto, angulado o de doble luz con guías regulares; posteriormente, en caso de imposibilidad de acceso, se pasó una guía específica de oclusión crónica con el microcatéter recto tras una modificación muy marcada de la forma del extremo distal de la guía.
Resultados: En nueve pacientes no se consiguió el acceso a la rama lateral con la estrategia inicial, en tres de ellos por imposibilidad de acceso y en los seis restantes por prolapso de la guía al intentar progresar el microcatéter. En todos los casos el acceso pudo completarse con una guía Gaia First, que combina un excelente torque con una rigidez suficiente para evitar el prolapso. Todos los procedimientos se realizaron sin complicaciones.
Conclusiones: El intervencionismo percutáneo en las ramas laterales con una marcada angulación puede conllevar una gran dificultad para el acceso con la guía. Estos procedimientos pueden realizarse de forma fácil y rápida con una guía específica de oclusión crónica.
Palabras clave: Bifurcación. Guía intracoronaria. Lesión angulada. Oclusión crónica.
Introduction
At times, using intracoronary guides to access sharply angulated lateral branches with a lesion that requires protection when treating bifurcations is extremely difficult. There is not too much information in the medical literature on the number of branches that cannot be accessed, but experienced groups say that the rate is around 3%1. Accessing the lateral branch is usually easy when the angle between the main branch and the lateral branch is < 70°, more difficult with distal bifurcation angles > 70º, and especially difficult with angles > 90°.
Different techniques and devices have been designed such as angulated microcatheters, double-lumen catheters2 or deflectable catheters2 o defectables3,4, which, combined with the use of hydrophilic guidewires allow us to be able to perform procedures. However, even when access has not occurred, the prolapse of the guidewire towards the main branch is a common thing when advancing the guidewire or the microcatheter, especially when dealing with sharp angles and large caliber main branches.
We hereby present a way to conduct this kind of procedure using a specific chronic occlusion guidewire that combines excellent maneuverability with great support in its distal edge to avoid prolapse. Additionally, we will be reviewing the different techniques and devices available today to perform these procedures.
Methods
Between January 2017 and October 2018, we analyzed patients with an indication for percutaneous intervention in their lateral branches or branches requiring a second guidewire when treating a bifurcation whose origin had a ≥ 80° angle through visual assessment. In all cases, the initial strategy was to use one Caravel microcatheter (Asahi, Japan) with the Sion and Fielder XT guidewires followed by the Stride angulated microcatheter (Teleflex, United States) or the Crusade double-lumen microcatheter (Kaneka, Japan).
In those cases where the guidewire advanced successfully with such devices, the Gaia First guidewire (Asahi, Japan) with the Caravel microcatheter was used. This guidewire was picked because of its excellent maneuverability, capacity to maintain the shape of its distal edge and the support granted by its distal segment. The characteristics of the procedures conducted with the Gaia First guidewire as well as the properties of this guide are described here because, in our opinion, they can be of great help in these cases.
Results
During the entire period of the study, 1342 percutaneous coronary interventions (PCIs) were conducted at our center, and in 52 (3.8%) of them, the lesion was found in a lateral branch whose origin had a ≥ 80° angle or was a bifurcation with an oversized lateral branch and the mentioned exit angle. In nine patients we were not able to access the lateral branch using the Sion or the Fielder XT guidewires and straight, angulated, or double-lumen microcatheters; in three cases it was due to the fact that we could not access using the guidewire distal edge, and in the remaining six because the main vessel prolapsed when trying to advance the guidewire or the microcatheter. All procedures were conducted using 6-Fr catheters, eight of them using the radial approach and the remaining one using the femoral approach. Table 1 shows the characteristics of the different cases.
Table 1. Characteristics of patients and lesions
| Age (years) | Bifurcation | Location | Indication of guidewire in lateral branch | Previous microcatheter | Angle | |
|---|---|---|---|---|---|---|
| Case 1 | 58 | LAD-diagonal | Diagonal | Protection | Angulated + double lumen | 80º |
| Case 2 | 53 | CX-OM1 | OM1 | Percutaneous interventionism | Angulated | 80º |
| Case 3 | 71 | CX-OM1 | OM1 | Protection | Angulated + double lumen | 100º |
| Case 4 | 80 | LAD-diagonal | Diagonal | Protection | Angulated | 100º |
| Case 5 | 60 | LAD-diagonal | Diagonal | Percutaneous interventionism | Angulated + double lumen | 100º |
| Case 6 | 53 | CX-OM1 | OM1 | Protection | Double lumen | 90º |
| Case 7 | 64 | LAD-diagonal | Diagonal | Protection | Angulated | 100º |
| Case 8 | 55 | LAD-diagonal | Diagonal | Percutaneous interventionism | Angulated + double lumen | 100º |
| Case 9 | 76 | Trunk-CX | CX | Percutaneous interventionism | Angulated | 120º |
|
CX, circumflex artery; LAD, left anterior descending artery; OM1, obtuse marginal. |
||||||
The last step that was successful in all the patients consisted of using the Caravel straight microcatheter and the Gaia First guidewire after modifying the shape of the tip to make it match the angle of the vessel (figure 1). Thanks to its excellent maneuverability and the support granted by its distal edge, this guidewire allows easy access to the vessel and facilitates the advance of the microcatheter so that we can change this guide by another guidewire with a softer tip. No coronary dissections, or vessel occlusions were reported, and all procedures were completed with optimal results.
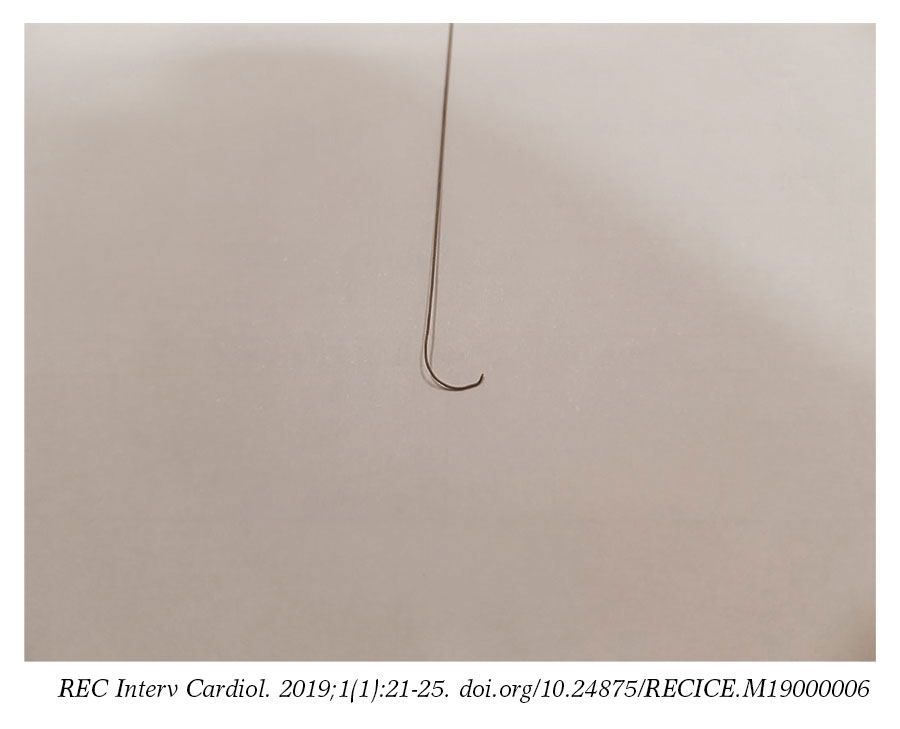
Figure 1. Modification of the Gaia First guidewire tip.
Video 1 of the supplementary data shows a case with a sharply angulated origin in a dominant circumflex artery of a very high-risk patient with a 25% ejection fraction who suffered from an anterior infarction back in 2002. The left anterior descending artery had a chronic occlusion of 50 mm in length with a scab in its anterior side. The procedure was conducted using the Impella CP ventricular assist device (Abiomed, United States) and the circumflex artery was accessed using the Gaia First guidewire and the aforementioned technique after trying the Sion and Fielder XT guidewires and one angulated microcatheter. Two 2 × 15 mm Resolute Onix stents (Medtronic, United States) were implanted at the beginning of the circumflex artery with optimal angiographic results (video 2 of the supplementary data). The patient was discharged three days after the uneventful implantation of a triple chamber defibrillator.
Figure 2 and figure 3 show two cases with double angulation with unsuccessful access using conventional guidewires; and figure 4 and figure 5, show two cases where the problem was the prolapse of the tip of the guidewire when trying to advance the guidewire or the microcatheter.
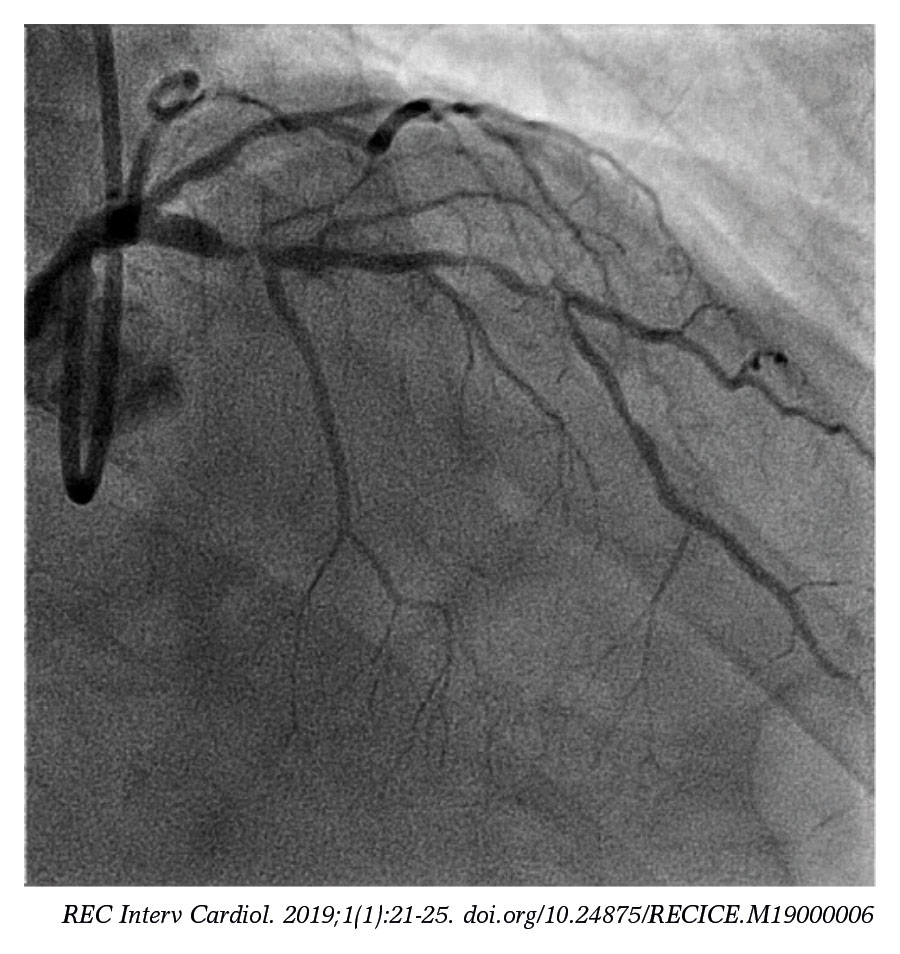
Figure 2. Access to the distal anterior descending artery, with a severe lesion, double angulation and diagonal bifurcation in the middle segment. Filed access with conventional guidewires and microcatheters.
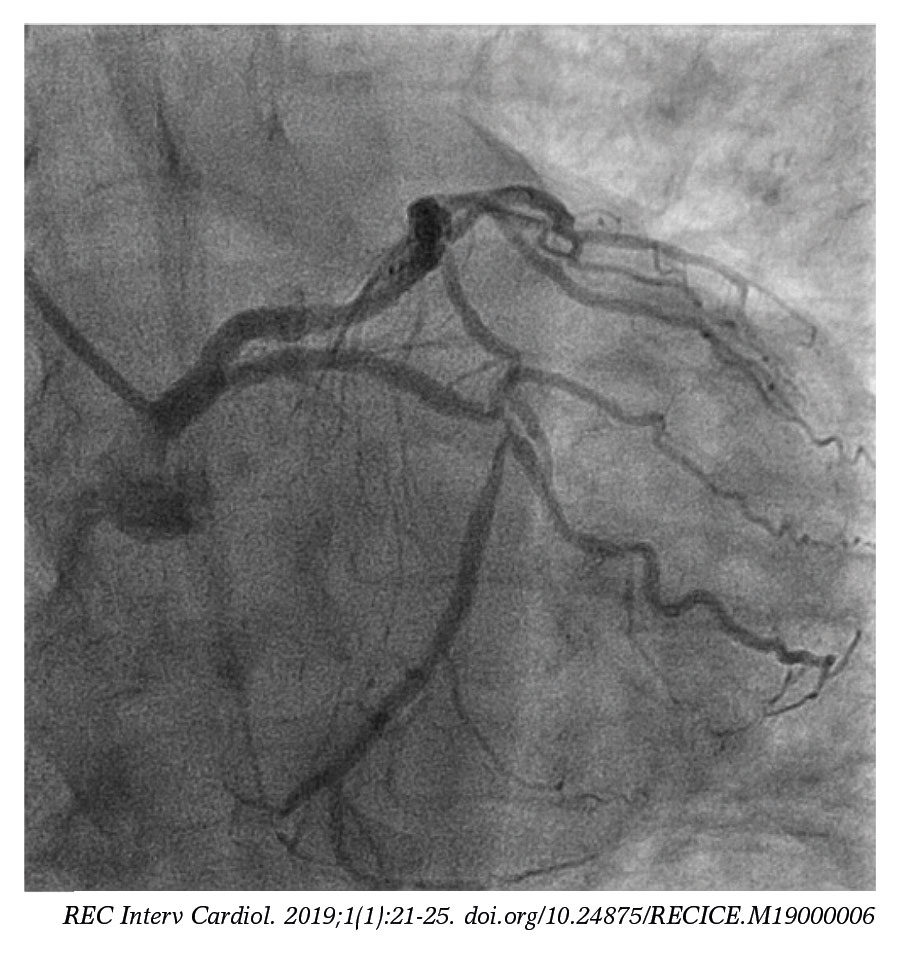
Figure 3. Access to the distal circumflex artery with double bifurcation and double angulation in the middle segment. Failed access with conventional guidewires and microcatheters.
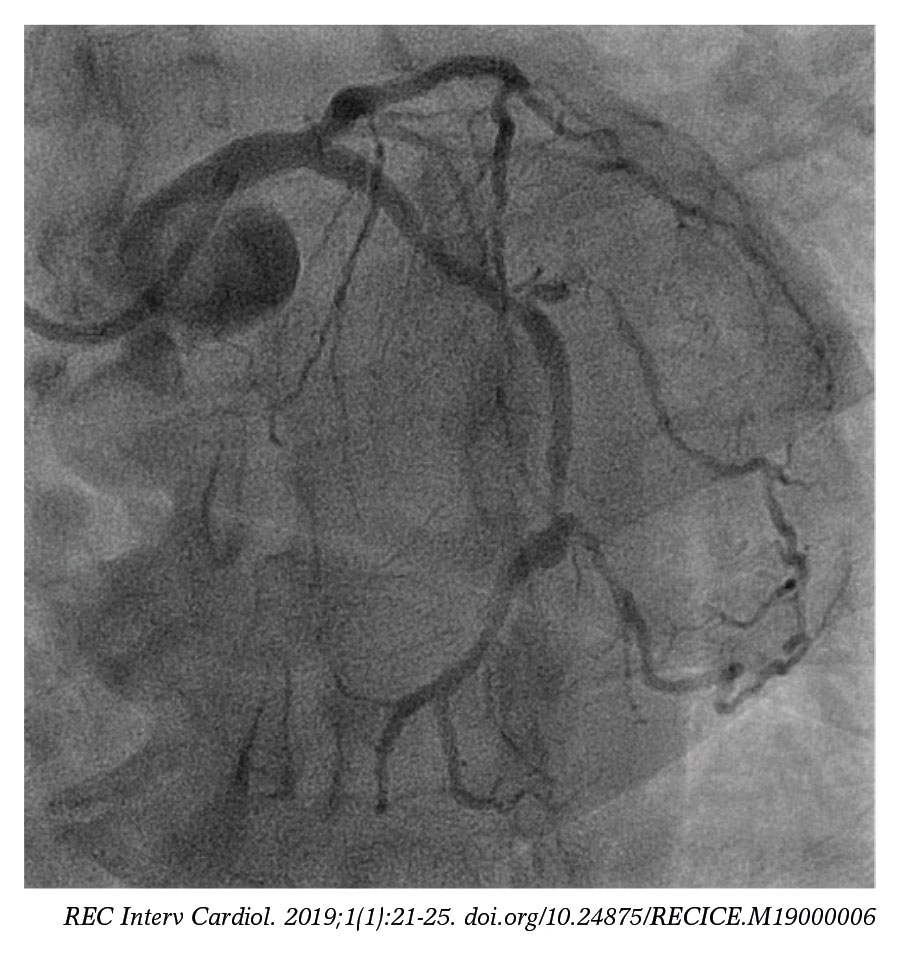
Figure 4. Access to the second marginal obtuse artery with double angulation. It was accessed using a conventional guidewire but repeated prolapse occurred when trying to advance the guidewire.
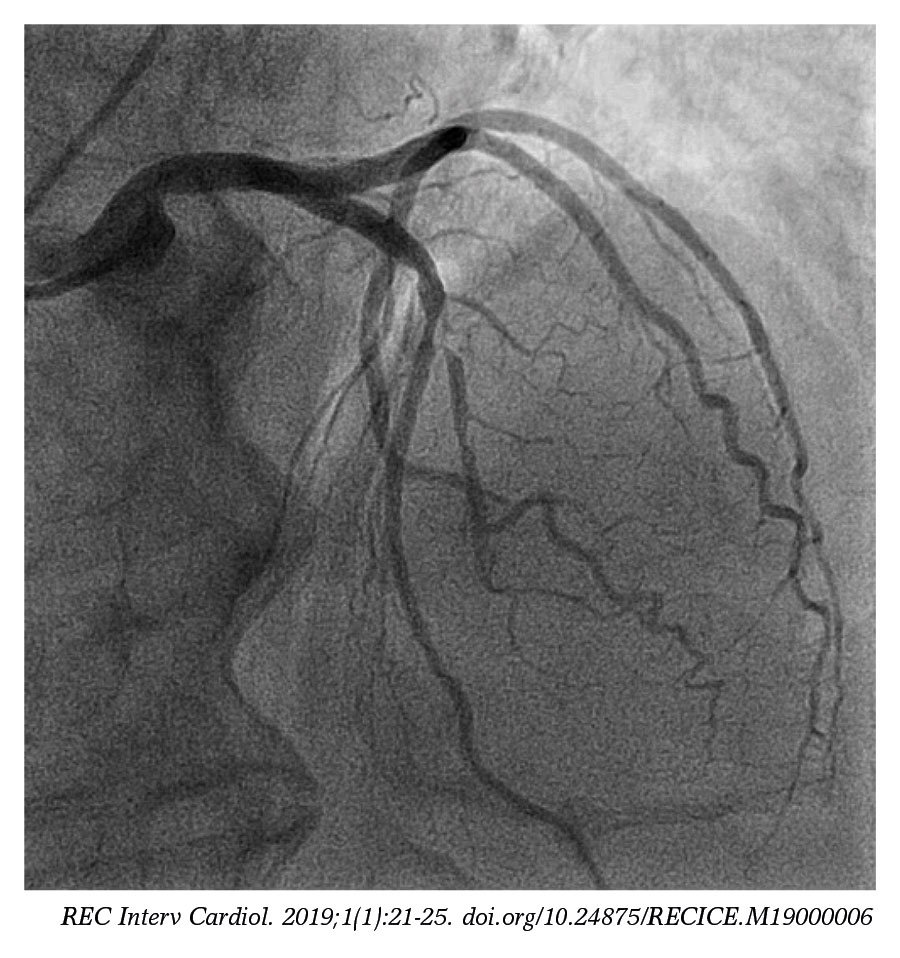
Figure 5. Access to the diagonal with angulated origin. It was accessed using a conventional guidewire but repeated prolapse occurred when trying to advance the guidewire.
Discussion
Accessing sharply angulated lateral branches with intracoronary guidewires can be difficult. To be able to solve this problem, several options5, have been described, among these, shaping the curvature of the tip of the guidewire, using guidewires with hydrophilic or more rigid polymeric coating, the double guidewire technique, inflating the balloon inside the main branch to modify the access, and use microcatheters with different designs (angulated, double-lumen, or deflectable).
The tip of the guidewire should have an adequate shape to facilitate access to the lateral branch. The curves typically used to access bifurcations are basically four: one single curve with a short tip (2-3 mm), one single curve with a long tip (4-6 mm), one single curve without rough angulation, and a double curve6. The latter are the most suitable shapes in cases of sharp angulations.
This study details the use of a guidewire designed for chronic occlusions7 and facilitate access to sharply angulated branches. The Gaia First guidewire, same as it happens with the Gaia Second and Third guidewires was first introduced into the market back in 2014. Seventeen years after its manufacturer, Asahi, would develop the very first prototype of specific guidewires for the management of chronic occlusions, the Miracle guidewire. Its design includes the 400 mm long SLIP-COAT coating that improves maneuverability inside the microcatheter with a distal coil structure of 150 mm, a 0.010” diameter and a load of 1.7 g on the tip. Such a design enables an excellent 1:1 capacity of manipulation which, in turn, helps maneuver the guidewire under optimal conditions. Although it was designed for the management of chronic occlusions, its perfect maneuverability of the tip added to how rigid the 150 mm distal segment is, and its capacity to maintain the shape of the tip make it an excellent guidewire for the access of sharply angulated branches granting the right support for the advancement of the microcatheter. We think it is important to say that this strategy used as a fist choice strategy after the hydrophilic guidewire has failed added to a straight microcatheter, can be very attractive financially since we do not need to use any additional curved, double-lumen, or deflectable microcatheters. However, we should not forget that although no complications were reported in the series described, the number of cases is limited and we always have to bear in mind that, even though it is a guidewire of limited lightweight and excellent maneuverability, it was designed for the management of chronic occlusions, so it should be used with care due to the theoretical risk of dissection or occlusion of the blood vessel.
There are other guidewires specifically designed for this type of lesions such as the Sion Black (Asahi, Japan), but, since this guidewire was not used in the lesions presented in this series, we cannot give any information on how it may behave in cases like the one presented here. Also, it is very difficult to have access to all the guidewires available in the market today and the goal of this study was to give an alternative solution when the first intention guidewires fail.
Another technique is the retrograde access to the lateral branch by giving the lateral branch guidewire much more curvature and trying to access the branch when the guidewire has been removed8. This is a sophisticated technique when using doublelumen microcatheters since we insert one hydrophilic guidewire whose very curved distal edge stands out through the lateral orifice of the microcatheter2,9-12. The idea is almost the same, to advance the double-lumen catheter over the guidewire located in the monorail compartment while the guidewire tries to access the lateral branch located in the coaxial compartment and standing out 5 mm to 10 mm through the lateral orifice and with the curve oriented almost 180º with respect to the main vessel. This way, when removing the microcatheter, we should be able to access the lateral branch using the bent guidewire.
We can also use the Venture deflectable catheter (Teleflex, United States) -compatible with e 6-Fr guidewire catheter- available in coaxial and monorail design, that allows us to use any 0.014” coronary guidewires.4,13. The 8 mm distal tip is radiopaque and it can bend up to 90º rotated with clockwise torque in the catheter proximal area. In order to avoid any traumas, it is advanced towards the lesion over a guidewire in straight position and, once the point of interest has been reached, the tip starts to bend until it reaches the target angle. This deflection capability added to the possibility of turning the tip of the catheter in a circumferential plane, allows us to direct the guidewire and, once it has passed, rotate it in the counterclockwise direction to make the catheter return to its straight position and then be able to remove it.3. The rate of success when accessing lateral branches is said to be close to 80%-85%3,4, and the rigidity of the tip requires being extremely careful to limit the possibility of traumatizing the vessel. A few cases of destructured guidewire due to over-manipulation have been reported.
Finally, it has also been suggested that we should inflate a balloon inside the bifurcation in order to change the plaque and allow access to the branch14, but this solution should only be used when the other solutions have failed because, although it is easy to do, previous dilatations can cause changes in the plaque and eventually lead to occluding the branch15.
Conclusions
Accessing sharply angulated lateral branches is very hard to do with the guidewire, at times, because the access site will not allow it, or due to posterior prolapse towards the main vessel. On top of angulated, double-lumen, or deflectable microcatheters with routine guidewires, these procedures can be performed easily using a specific guidewire for the management of chronic occlusions that combines the excellent maneuverability of the tip and support of the distal edge which facilitates the advancement of the straight microcatheter to later change the guidewire for another guidewire with a softer distal edge.
Conflicts of interests
No conflicts of interest declared whatsoever.
Supplementary data
Video 1. Lozano I. DOI: 10.24875/RECICE.M19000006
Video 2. Lozano I. DOI: 10.24875/RECICE.M19000006
What is known about the topic?
- Accessing sharply angulated lateral branches is usually very difficult. Different techniques and devices have been designed such as angulated micro-catheters, double-lumen catheters or deflectable catheters to make these procedures easier, but even when access has been successful, there are times when we witness the prolapse of the guidewire towards the main branch when advancing the guidewire or the microcatheter, especially with sharply angulated origin branches and large caliber main branches.
- Over the last few years, we have witnessed the arrival of new intracoronary guidewires, especially those for the management of chronic occlusions.
What does this study add?
- The applicability of the Gaia First guidewire was presented here for the first time. Also, its particular characteristics of excellent maneuverability, easy advancement thanks to its high-quality hydrophilic coating, and moderate support of its distal edge. All these features make it an excellent tool to access sharply angulated lateral branches.
- The Gaia First guidewire gives us an easy, highly effective, fast technique to be able to perform complex interventions when we need to access sharply angulated lateral branches.
- The series described is short and from one single center only but, if we could confirm these results in a larger multicenter series and, therefore, extrapolate these results, the Gaia First guidewire could become the first choice guidewire; also, this would save costs since we would be getting rid of all of the aforementioned microcatheters that are usually the second options when the straight microcatheter has failed.
References
1. Pan M, Suarez de Lezo J, Medina A, et al. Drug-eluting stents for the treatment of bifurcation lesions:a randomized comparison between paclitaxel and sirolimus stents. Am Heart J. 2007;153:15e1-7.
2. Lee HF, Chou SH, Tung YC, Lin CP, Ko YS, Chang CJ. Crusade Microcatheter-Facilitated Reverse Wire Technique for Revascularization of Bifurcation Lesions of Coronary Arteries. Acta Cardiol Sin. 2018;34:31-36.
3. McClure SJ, Wahr DW, Webb JG. Venture wire control catheter. Catheter Cardiovasc Interv. 2005;66:346-350.
4. Ojeda S, Pan M, Mazuelos F, et al. Use of the venture wire-control catheter for accessing side branches during provisional stenting:an option for bifurcations with an unfavorable anatomy. Rev Esp Cardiol. 2010;63:1487-1491.
5. Cortese B, Limbruno U. Coronary bifurcation lesions:innovative approaches and the future of bifurcation devices. Future Cardiol. 2010;6:221-230.
6. Burzotta F, De Vita M, Sgueglia G, Todaro D, Trani C. How to solve difficult side branch access? EuroIntervention. 2010;6:J72-80.
7. Khalili H, Vo MN, Brilakis ES. Initial Experience With the Gaia Composite Core Guidewires in Coronary Chronic Total Occlusion Crossing. J Invasive Cardiol. 2016;28:E22-25.
8. Kawasaki T, Koga H, Serikawa T. New bifurcation guidewire technique:a reversed guidewire technique for extremely angulated bifurcation — a case report. Catheter Cardiovasc Interv. 2008;71:73-76.
9. Nomura T, Higuchi Y, Kato T. Successful percutaneous coronary intervention for complex bifurcated lesions with combination of “Reverse wire technique“and “Reverse bent wiring with the crusade catheter“ novel wire manipulation technique. Catheter Cardiovasc Interv. 2016;87:920-925.
10. Nomura T, Higuchi Y, Kubota H, et al. Practical Usefulness of Dual Lumen Catheter-Facilitated Reverse Wire Technique for Markedly Angulated Bifurcated Lesions. J Interv Cardiol. 2015;28:544-550.
11. Nomura T, Kikai M, Hori Y, et al. Tips of the dual-lumen microcatheter-facilitated reverse wire technique in percutaneous coronary interventions for markedly angulated bifurcated lesions. Cardiovasc Interv Ther. 2018;33:146-153.
12. Suzuki G, Nozaki Y, Sakurai M. A novel guidewire approach for handling acute-angle bifurcations:reversed guidewire technique with adjunctive use of a double-lumen microcatheter. J Invasive Cardiol. 2013;25:48-54.
13. Lilli A, Vecchio S, Giuliani G, et al. Venture wire control catheter in percutaneous treatment of complex coronary bifurcation. A case report. Minerva Cardioangiol. 2008;56:255-258.
14. He X, Gao B, Liu Y, Li Z, Zeng H. Side-branch technique for difficult guidewire placement in coronary bifurcation lesion. Cardiovasc Revasc Med. 2016;17:59-62.
15. Chen SL, Louvard Y, Runlin G. Perspective on bifurcation PCI. J Interv Cardiol. 2009;22:99-109.












