
While performing aortic valve-in-valve procedures the fracture of certain surgical biological valve annuli has been widely reported regarding the implantation of a larger percutaneous valve with a better hemodynamic profile. The pulmonary valve-in-valve technique has not been around that much, but its role is more important because it allows «small» valve implantation in pediatric patients who later progress into significant somatic growths. We present 2 cases after obtaining the express consent of the patients or, if minors, of their legal tutorss.
Case #1 is a 15-year-old patient with Fallot’s tetralogy, and previous surgical implantation of a 19 mm Carpentier Magna Ease valve (Edwards Lifesciences Corp., United States) (internal lumen of 17 mm) at 11 years old. Severe stenosis and moderate regurgitation. The annulus ruptured with a 20 mm x 20 mm Atlas Gold balloon (Becton, Dickinson and Company Franklin Lakes, United States) inflated at 22 atm, and a 23 mm Edwards S3 valve was implanted (figure 1A, angiography of pulmonary artery; figure 1B, rupture with balloon; figure 1C, previous ruptured valve [arrow]; figure 1D, new valve; and videos 1-4 of the supplementary data).
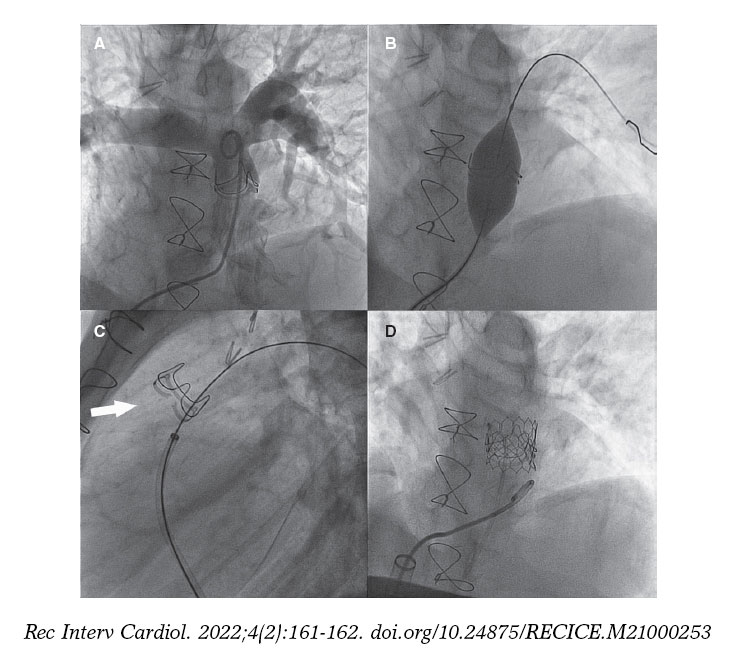
Figure 1.
Case #2 is a 24-year-old patient with Fallot’s tetralogy and previous surgical implantation of a 21 mm Carpentier Edwards valve (internal lumen of 19 mm) at 14 years old. Moderate doble lesion. The valve ruptured with a 24 mm x 20 mm Atlas Gold balloon inflated at 20 atm, and a 26 mm Edwards XT valve was implanted (figure 2A, angiography of pulmonary artery; figure 2B, rupture with balloon; figure 2C, previous ruptured valved distended with a 25 mm Cristal balloon (Balt, France) [arrow]; figure 2D, new valve; and videos 5-8 of the supplementary data).
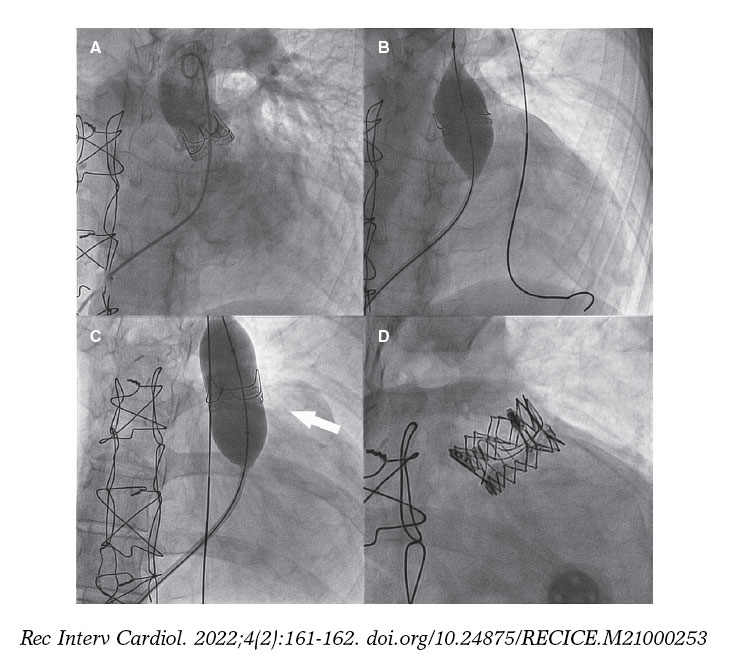
Figure 2.
The rupture of a biological prosthetic valve annulus in pulmonary position facilitates the implantation of another larger valve to match the growth of each patient, and makes valve-in-valve procedures possible in the future. This procedure can be unnecessary if the first prosthetic valve implantation is performed with long-term thinking and the largest possible valve is used.
FUNDING
None whatsoever.
AUTHORS’ CONTRIBUTIONS
The 3 authors participated in the idea, writing, and review of this article.
CONFLICTS OF INTEREST
None reported.
SUPPLEMENTARY DATA
Vídeo 1. Betrián Blasco P. DOI: 10.24875/RECICE.M21000253
Vídeo 2. Betrián Blasco P. DOI: 10.24875/RECICE.M21000253
Vídeo 3. Betrián Blasco P. DOI: 10.24875/RECICE.M21000253
Vídeo 4. Betrián Blasco P. DOI: 10.24875/RECICE.M21000253
Vídeo 5. Betrián Blasco P. DOI: 10.24875/RECICE.M21000253
Vídeo 6. Betrián Blasco P. DOI: 10.24875/RECICE.M21000253
Vídeo 7. Betrián Blasco P. DOI: 10.24875/RECICE.M21000253
Vídeo 8. Betrián Blasco P. DOI: 10.24875/RECICE.M21000253












