
This is the case of an 83-year-old man with symptomatic, severe aortic valve stenosis referred for transcatheter aortic valve implantation (TAVI). The echocardiogram revealed the presence of a severely calcified stenotic aortic valve (0.6 cm2) with bicuspid anatomy (figure 1A). The computed tomography scan revealed an Agatston calcium score of 17 727 (figure 1B), a 30 mm aortic annulus diameter, and dilated aortic root and aortic angulation > 70º (figure 1C). Aortography was performed (figure 1D).
Crossing the aortic valve with a guidewire for 60 min using catheters of various curves/sizes and several types of guidewires (with or without J-shaped tip, whether hydrophilic or not) was attempted by 2 highly skilled operators. Strategy, then, changed and a XB4 6F left coronary guide catheter (Cordis, United States) was used to manipulate a 0.014 inch hydrophilic Pilot 50 intracoronary guidewire (Abbott, United States) that easily crossed the aortic valve (figure 1E). A 6-Fr guide catheter extension system (Deeper, IHT-Cordynamic, Spain) was mounted on the wire and advanced to the left ventricular apex (figure 1F). Afterwards, the intracoronary guidewire was replaced by a 0.035 inch extra-stiff guidewire by removing both the guide and extension catheter systems (figure 1G). This original new approach took just 5 min.
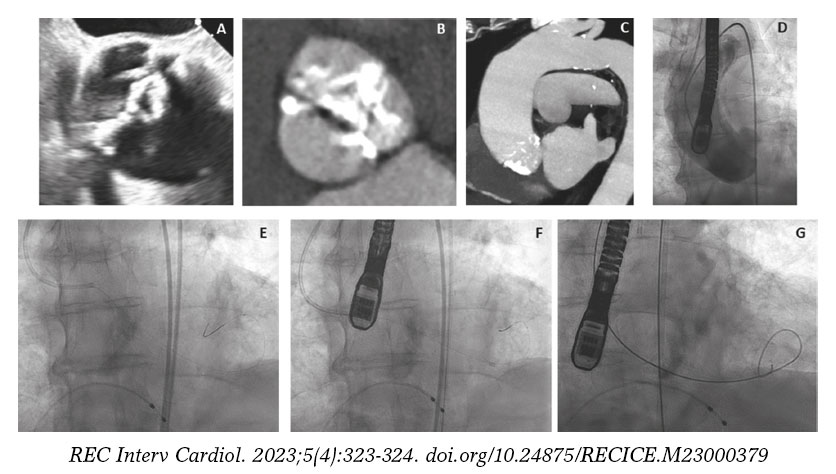
Figura 1
The impossibility of crossing the aortic valve with a guidewire is rare. In our case the difficulty was due to a severely stenotic valve with massive calcification, bicuspid morphology, horizontal aorta, and dilatation of both the aortic root and the annulus.
This case is a truly original and novel technique, simple and safe, to achieve the guidewire crossing of a very stenotic aortic valve with a complex anatomy. This technique illustrates the cross-over use of coronary and structural interventional tools to solve complex problems.
Consent was obtained from the patient for the publication of this case.
FUNDING
None reported.
AUTHORS’ CONTRIBUTIONS
All authors contributed to data collection, drafting, review, and approval of the manuscript.
CONFLICTS OF INTEREST
J. M. de la Torre-Hernández is editor-in-chief of REC: Interventional Cardiology. The journal’s editorial procedure to ensure impartial handling of the manuscript has been followed. The other authors do not declare any conflict.












