
A 59-year old male with severe left ventricular dysfunction, slow ventricular tachycardia and previously treated with cardiac resynchronization therapy was referred for percutaneous coronary intervention (PCI) of the left anterior descending coronary artery (LAD). The patient had 2 severely calcified lesions at mid-LAD level. Because it was a high-risk PCI, the heart team decided to perform this procedure using percutaneous left ventricular support using the Impella CP device (Abiomed, United States). The patient had a past medical history of right femoral-popliteal bypass surgery and a severely calcified stenosis in his left external iliac artery (figure 1A, arrow). The computed tomography performed on the supraaortic arteries revealed subclavian and axillary arteries with diameters < 5mm (figure 1B). The Impella CP device (14-Fr)—that requires a minimal vessel diameter of 5mm—was implanted using the left femoral access after revascularization of left external iliac artery. Predilation was performed using a 5 x 40 mm Mustang PTA balloon catheter (Boston Scientific, United States) (figure 1C); afterwards a 6 x 38 mm balloon expandable covered stent Advanta V12 (Atrium Medical Corporation, United States) was implanted (figure 1D,E). The Impella CP device was advanced through the stent (figure 1F). The PCI of the mid-LAD was performed using 2 drug-eluting stents (figure 1G,H; arrows: lesions at mid-LAD level). After the PCI, the Impella CP device was retrieved; vascular access was closed using Perclose ProGlide (Abbott Vascular Inc., United States). The control angiography showed good results (figure 1, video 1 of the supplementary data).
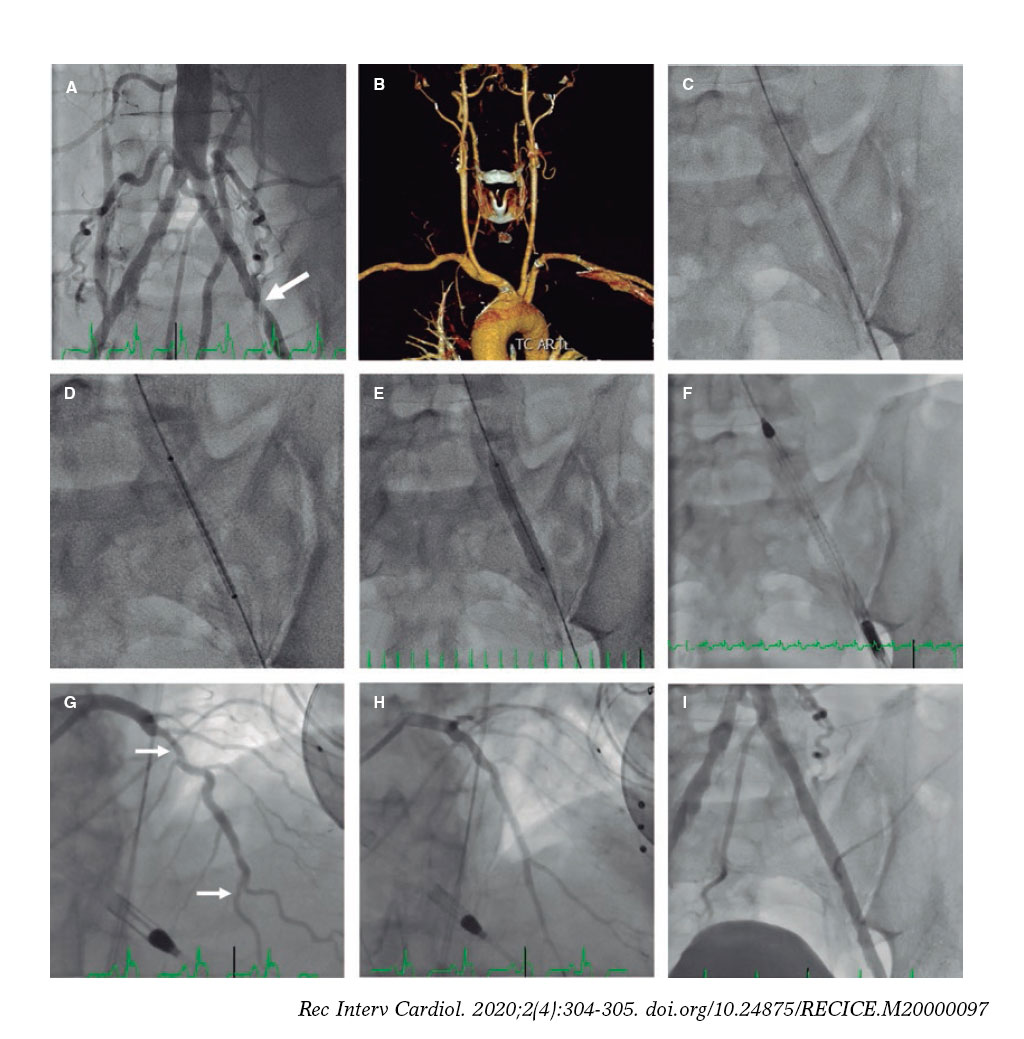
Figure 1.
The percutaneous revascularization of the iliac artery with a covered stent may be an alternative approach to advance the Impella CP device and facilitate high-risk PCIs when subclavian and axillary accesses are not an option for having small diameters.
SUPPLEMENTARY DATA
Video 1. Cubero-Gallego H. DOI: 10.24875/RECICE.M20000097












