
This is the case of a 53-year-old man with aortic stenosis, ascending aortic aneurysm, and type B aortic dissection treated with Bentall procedure where a 40 mm uncovered self-expanding stent-graft (AMDS, JOTEC GmbH, Germany) was anastomosed to the aortic graft distal border with the intent to collapse the entry (figure 1A). The patient’s written informed consent was obtained to run the tests and publish the case.
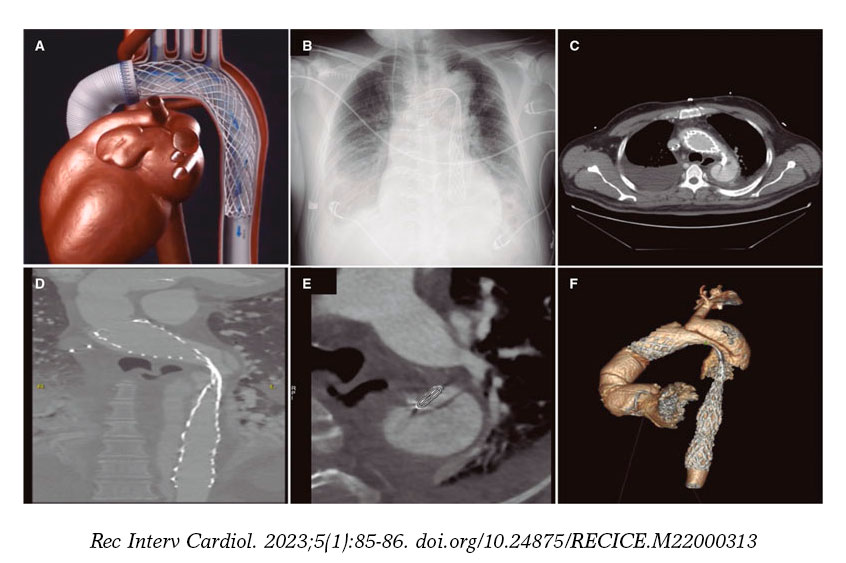
Figure 1.
The follow-up radiographic monitoring revealed significant stent-graft kinking while the dissection entry remained opened (figure 1B,F).
Given the high risk involved in the reintervention, endovascular treatment was decided. Under intravascular echocardiography guidance a hydrophilic guidewire was used to cross the stent-graft lumen. Afterwards, the guidewire was exchanged for a different one with stronger support to proceed with dilatations using semi-compliant balloons with significant recoil being reported after balloon deflation (figure 2A,C).
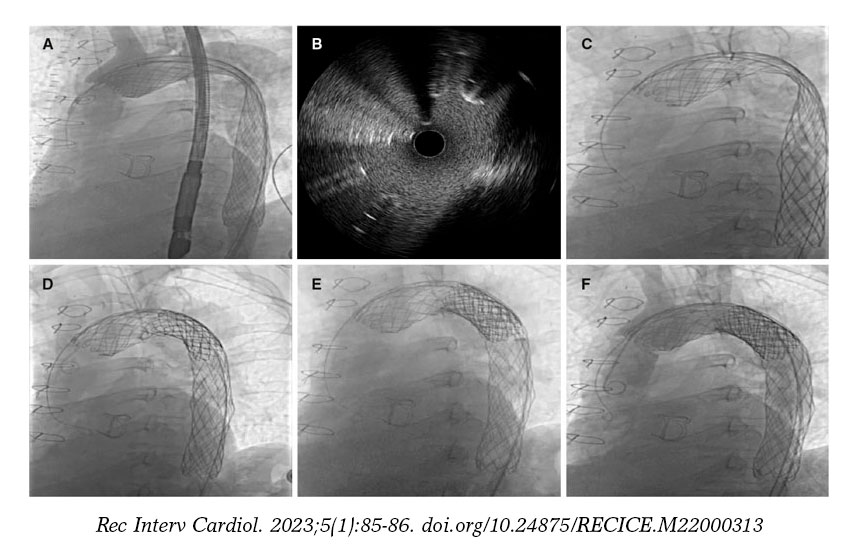
Figure 2.
To achieve greater radial strength, we decided to implant a double-layer stent. An uncovered stent to expand the stent-graft was implanted followed by 1 covered expandable polytetrafluoroethylene (e-PTFE) stent to seal the dissection entry. An 18 Fr DrySeal sheath (Gore Inc, United States) was used to implant 2 60 mm 10-zig CP stents (NuMED Inc, United States), 1 covered and the other one not. Both stents were mounted on a 26 mm × 50 mm BIB balloon (NuMED Inc., United States). A 30 mm × 60 mm Crystal balloon (BALT, Germany) was used for postdilatation (figure 2D,E). The control computed tomography scan confirmed the dissection entry complete seal with persistent distal false lumen (figure 3A,D).
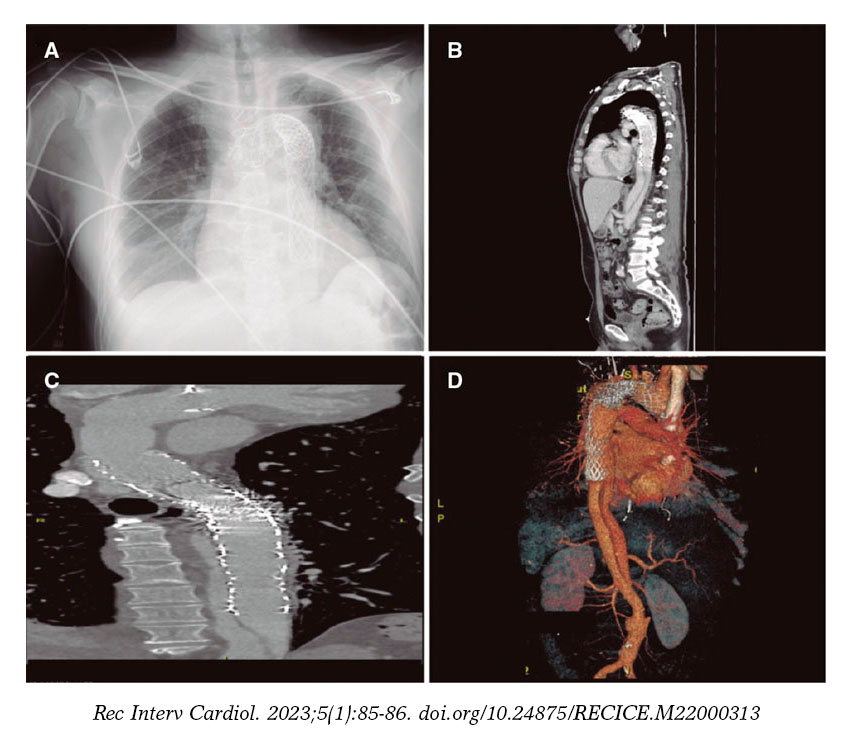
Figure 3.
FUNDING
None whatsoever.
AUTHORS’ CONTRIBUTIONS
All authors contributed equally to this work.
CONFLICTS OF INTEREST
None reported.
* Corresponding author.
E-mail address: luisfg82@hotmail.com (L. Fernández González).










