
CASE RESOLUTION
The patient was referred to the cath lab. The high left brachial artery access was tried using the dissection technique due to significant stenosis of the distal brachial artery as a consequence of an aortography performed during the patient’s childhood with the Sones technique. General anesthesia with selective orotracheal intubation was used. A 6-Fr Cobra-type guide catheter was advanced and entered the pseudoaneurysm. An early injection was used for its catheterization (video 1 and video 2 of the supplementary data) (neck: 8.4 mm; base: 2.9 x 1.5 cm). Three fiber coils (6 mm with 5 turns) were deployed in the base of the pouch (figure 1). Afterwards, a 5 x 4 mm Amplatzer ADO II device was positioned and delivered in the pseudoaneurysm neck. The persistence of the passage of contrast to the pouch was evident and it was decided to deliver another 6.5 mm fiber coil with 3 turns to finish the pseudoaneurysm neck sealing (figure 2, video 3 of the supplementary data). One month after the procedure, the patient had a new episode of hemoptysis. The coronary computed tomography angiography performed confirmed the patency of the pouch in its proximal portion, which is why the patient underwent a second procedure. This time the procedure was performed under local anesthesia using the brachial dissection technique, a 6-Fr Cobra-type guide catheter, and pouch embolization with Interlock 2D coils of 20 and 8 cm. The complete filling of the pseudoaneurysm was secured (figure 3, video 4 of the supplementary data).
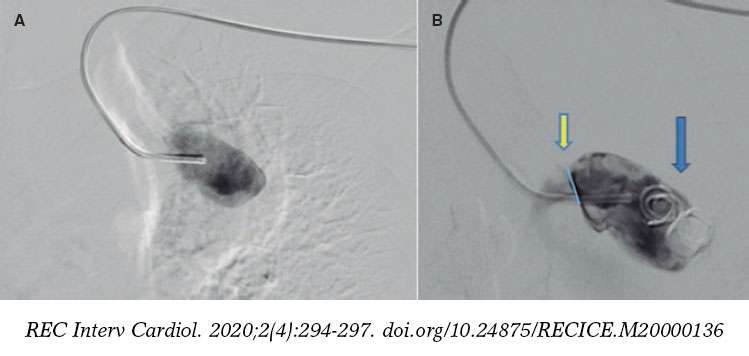
Figure 1. A: anteroposterior projection showing the trajectory of the catheter until it enters the pseudoaneurysm. B: right anterior oblique projection at 20º showing 3 fiber coils occupying a third of the base of the pouch (blue arrow); additionally, flowback is seen indicative of the pseudoaneurysm neck (yellow arrow).
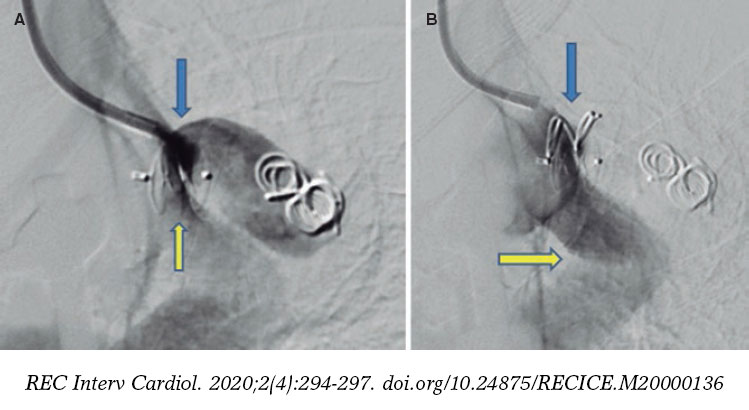
Figure 2. A: right anterior oblique projection at 20º showing the Amplatzer device partially sealing the neck (yellow arrow). An endoleak seen above the device that keeps filling the pseudoaneurysm (blue arrow). B: fiber coil sealing the endoleak (blue arrow) and subclavian-aortic bypass with Dacron graft (yellow arrow).
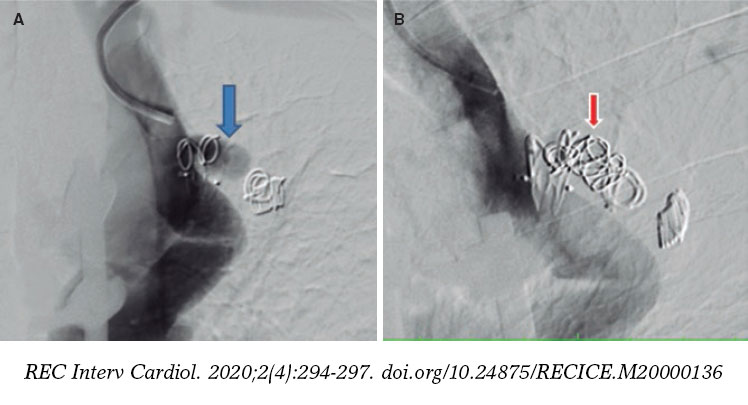
Figure 3. A: left anterior oblique projection at 20º. The blue arrow shows the endoleak partially filling the pouch. B: left anterior oblique projection at 30º. The red arrow shows the Interlock coils totally occupying the pouch.
Pseudoaneurysms are due to the rupture of 1 of the layers of the vessel wall that is contained by the remaining layers of the wall and adjacent structures. In general, it is often corrected through surgery. The endovascular resolution of this condition with the use of coils or other devices is not a common thing in the medical literature; however, it is a valid option for selected cases. This time, such technique was decided because of the urgent need to solve the case and considering the material and equipment available at our center. The use of covered stents to correct coarctations of aorta or interruptions of the aortic arch due to nearby aneurysms or pseudoaneurysms has been reported in the medical literature; however, in this particular case, the proximity of both subclavian arteries required a bilateral carotid-subclavian bypass before deploying the endoprosthesis followed by left subclavian artery embolization, which would delay the procedure.
SUPPLEMENTARY DATA
Video 1. García J. F. DOI: 10.24875/RECICE.M20000136
Video 2. García J. F. DOI: 10.24875/RECICE.M20000136
Video 3. García J. F. DOI: 10.24875/RECICE.M20000136
Video 4. García J. F. DOI: 10.24875/RECICE.M20000136












