
To the Editor,
Up until 2005, the percutaneous management of chronic total coronary occlusions was rare basically due to a low rate of success.1 This tendency started to change with the arrival of new materials and retrograde access techniques that improved the results of this procedure.2
The retrograde access technique is still being perfected and there is a growing number of promising strategies for the management of chronic total coronary occlusions.3 Retrograde access is often used with septal collaterals. Only in exceptional cases the epicardial collaterals are navigated due to a greater risk of perforation.4 However, in certain chronic total coronary occlusions of the left anterior descending artery (LAD), the homocoronary collateral vessels of the left circumflex artery (LCx) are often epicardial and require special care and use of a single vascular access.
We present the case of a 68-year old woman with a past medical history of high blood pressure, dyslipidemia, smoking, and hiatal hernia. She had functional class II/IV stable angina5 of 6-month duration. The myocardial perfusion scintigraphy confirmed the presence of anterior ischemia. The cine coronary arteriography showed a nondominant right coronary artery, a left main coronary artery without lesions, a LCx without lesions, and the total obstruction of the LAD in its proximal segment (figure 1). Our department/service was consulted because the recanalization attempt performed in another center was unsuccessful. While evaluating the case, a total occlusion was found in the proximal segment of the LAD without a stump and with a blunt edge. Other findings were the origin of the major diagonal branch at obstruction level—lesion apparently > 20 mm—and retrograde filling through the collateral circulation of the LCx. The J-CTO (Japanese Multicenter Chronic Total Occlusion Registry)6 calculated score was 3 (very difficult).
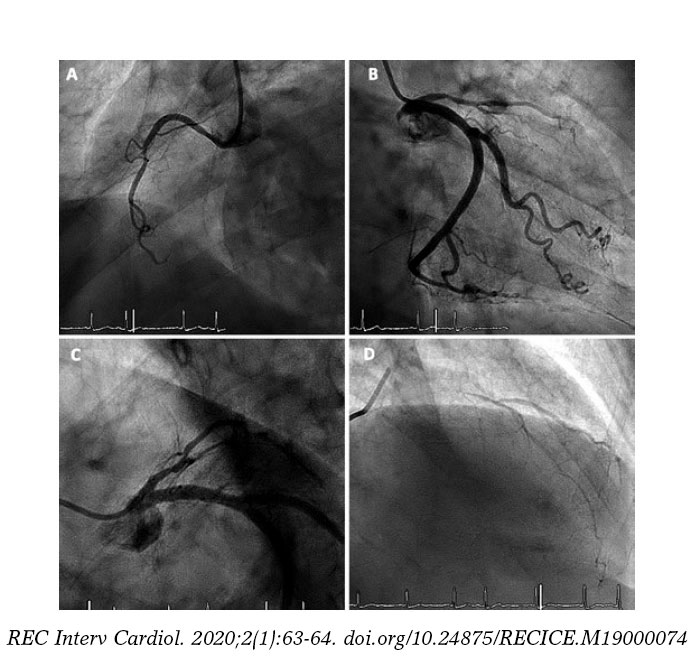
Figure 1. A: nondominant right coronary artery. B: circumflex artery without lesions. C: total occlusion in the anterior descending artery proximal segment without a stump and with a blunt edge. Origin of a major diagonal branch at obstruction level. D: anterior descending artery with retrograde filling through homocoronary collateral circulation.
Left radial puncture was performed (due to the absence of right radial pulse) using a 6-Fr radial sheath introducer. Selective catheterization was used in the left coronary artery with an XB 4 6-Fr guide catheter. Using the antegrade access a new recanalization attempt turned out unsuccessful. Since the patient showed no collateral circulation from the right coronary artery to the LAD, retrograde recanalization was decided through the collaterals of the LCx towards the LAD. The septal collateral branches of the LCx and LAD arteries were identified and a 0.014 in Sion Blue guidewire (Asahi Intec, Nagoya, Japan) was advanced mounted on a Corsair microcatheter (Asahi Intec, Nagoya, Japan). Collaterals were navigated and the LAD was recanalized using the retrograde access (figure 2). Also, using the retrograde access, the flexible part of the guidewire was reintroduced into the XB 4 catheter followed by the advancement of the Corsair microcatheter (tip-in technique7). The guidewire was removed leaving the Corsair catheter. The guide catheter was reintroduced and using a 0.014 in Cross-IT 200XT guidewire (Abbott, Abbott Park, Illinois, United States) through antegrade access the guidewire flexible tip was threaded with the Corsair distal edge inside the guide catheter. Then the guidewire was advanced. The Corsair device was removed, the LAD proximal lesion was predilated with a 1.5 x 20 mm-balloon and the angioplasty was completed using a 2.75 x 20 mm-XIENCE stent (Abbott, Abbott Park, Illinois, United States). The patient was referred to the outpatient surgery unit and discharged from hospital 6 hours later.
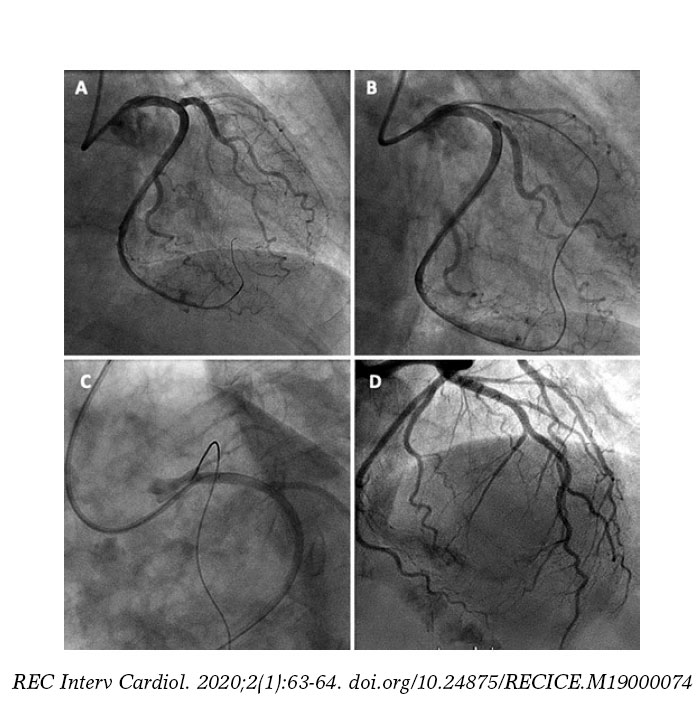
Figure 2. A: advancement of a 0.014 in Sion Blue guidewire through collaterals towards the anterior descending artery. B: retrograde recanalization of the anterior descending artery. C: reintroduction of guidewire and Corsair microcatheter inside the XB 4 guide catheter (tip-in technique). D: final angiography after stent implantation.
Although the homocoronary retrograde access can be performed using the double catheter technique—the so-called “ping-pong technique”8—facilitating the manipulation of materials through antegrade access, we chose a single arterial access since it is the less invasive option. However, it may interfere with the movement of materials in the antegrade direction (this limitation could improve with the use of 7-Fr catheters). In this case and even though we used a 6-FR guidewire we did not find any trouble moving the materials in the antegrade direction (using fewer materials also helped). Although feasible, this should be a last resource technique because of the greater risk involved in cases of perforations. In cases of very long total chronic coronary occlusions that require other techniques9 such as the controlled antegrade and retrograde subintimal tracking (CART), double vascular access is preferred because it requires materials of a lower profile. Coronary angioplasty through retrograde access has improved the rate of success of total chronic coronary occlusions.9 Although this technique is conceptually simple, it requires the appropriate tools and experienced heart teams to achieve optimal outcomes.
REFERENCES
1. Suero JA, Marso SP, Jones PG. Procedural outcomes and long-term survival among patients undergoing percutaneous coronary intervention of a chronic total occlusion in native coronary arteries:a 20-year experience. J Am Coll Cardiol. 2001;38:409-414.
2. Surmely JF, Tsuchikane E, Katoh O. New concept for CTO recanalization using controlled antegrade and retrograde subintimal tracking:the CART technique. J Invasive Cardiol. 2006;18:334-338.
3. Galassi A, Werner G, Boukhris M. Percutaneous recanalisation of chronic total occlusions:2019 consensus document from the EuroCTO Club. EuroIntervention. 2019;15:198-208.
4. Azzalini L, Brilakis ES. Ipsilateral vs. contralateral vs. no collateral (antegrade only) chronic total occlusion percutaneous coronary interventions:What is the right choice for your practice?Catheter Cardiovasc Interv. 2017; 89:656-657.
5. Kaul P, Naylor CD, Armstrong PW. Assessment of activity status and survival according to the Canadian Cardiovascular Society angina classification. Can J Cardiol. 2009;25:e225-231.
6. Morino Y, Abe M, Morimoto T, et al. Predicting successful guidewire crossing through chronic total occlusion of native coronary lesions within 30 minutes:the J-CTO (Multicenter CTO Registry in Japan) score as a difficulty grading and time assessment tool. JACC Cardiovasc Interv. 2011;4: 213-221.
7. Vo MN, Ravandi A, Brilakis ES. “Tip-in“technique for retrograde chronic total occlusion revascularization. J Invasive Cardiol. 2015;27:E62-64.
8. Koutouzis M, Avdikos G, Nikitas G. “Ping-pong“technique for treating a balloon uncrossable chronic total occlusion. Cardiovasc Revasc Med. 2018; 19:117-119.
9. Yamane M. Current Percutaneous Recanalization of Coronary Chronic Total Occlusion. Rev Esp Cardiol. 2012;65:265-277.












