
HOW WOULD I APPROACH IT?
The authors present an interesting and challenging case regarding percutaneous treatment, and with a very complex resolution. This is the case of a patient already surgically revascularized with significant ischemia whose revascularization option is through the bypass on which the entire territory of the left circumflex artery depends on.
At this point right now of the angioplasty where the stent cannot be crossed despite the use of the buddy-wire technique, and even though the stent was very short and had good navigability, I would try the following staged maneuvers:
1) Try to advance a high-support guidewire a little more distal inside the native vessel taking advantage of the native artery good distal bed so that the guidewire section with the highest support of all is placed on the curve zone. If possible, I would even bend the tip to avoid damaging the artery aware that the push forward maneuvers we’ll be performing can uncontrollably displace the guidewire at any time.
2) Benefit from the balloon already crossed and the lesion already dilated to redilate the lesion with the balloon using the anchorage technique with the balloon to move the guide extension catheter forward, cross the curve, and eventually reach the lesion. With the balloon properly inflated, fix, and pull the balloon hypotube back out while the guide extension catheter is smoothly and gently advanced deep into the artery (figure 1 and figure 2).
3) Once the guide extension catheter is at lesion entry level and to secure the crossing even further, I would use the buddy-wire technique to implant the short stent we already have after examining it to discard any damage during the previous maneuvers.
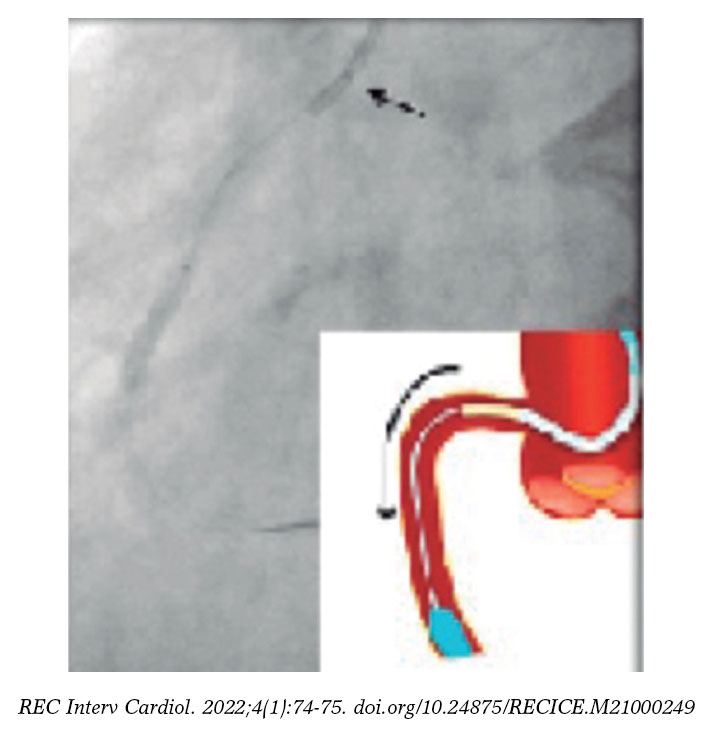
Figure 1. Example of anchorage inflating a balloon in the artery distal area and slightly pulling the hypotube back out to gently advance the guide extension catheter (in yellow).
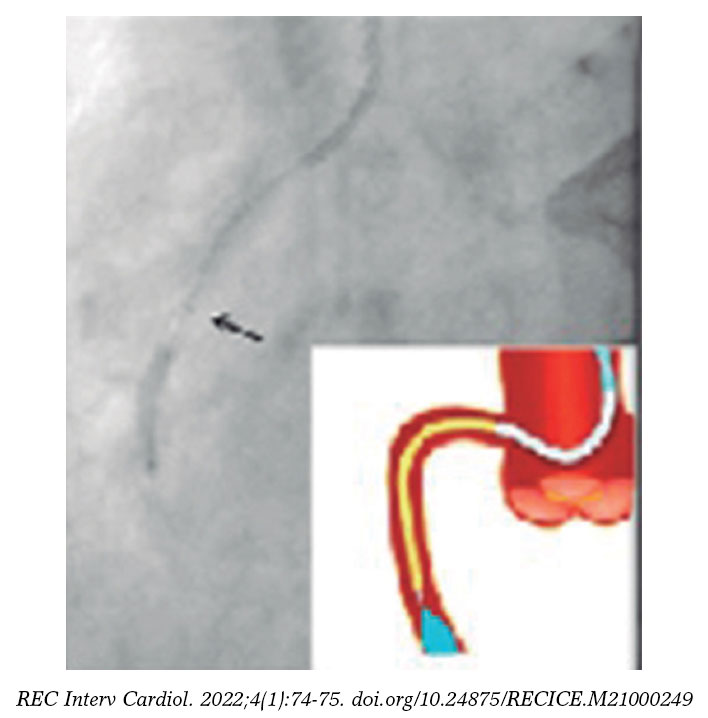
Figure 2. The guide extension catheter is advanced towards the lesion more proximal site, and the artery is deeply intubated, which increases support.
Although it is true that this deep intubation technique is widely used in native coronary arteries and was described some time ago,1,2 it should be used with extra care when dealing with bypasses, especially in the saphenous vein, to avoid dissecting or even perforating the saphenous vein bypasses that often appear degraded.
In this case the fact that the emergency of the saphenous vein bypass does not have a great proximal tortuosity and is properly aligned with the guide catheter used was an advantage.
Also, the type of guide extension catheter used should be carefully selected because there are many different ones available in the market. Some provide strength to give great support while others provide flexibility for deeper intubation without too much damage to the arteries.
FUNDING
None whatsoever.
CONFLICTS OF INTEREST
None reported.
REFERENCES
1. UnzuéL, Hernández F, Velázquez MT, García J, Albarrán A, Andreu J. Utilización del catéter GuideLiner®en angioplastias coronarias complejas. Rev Esp Cardiol. 2012;65:484-485.
2. Melado Corral S, UnzuéL, García E. Angioplastia simultánea a tres vasos con extensor de catéter GuideLiner®. Enferm Cardiol. 2018;25:78-79.
* Corresponding author: Sección de Hemodinámica, Hospital Universitario Lucus Augusti, Rúa Dr. Ulises Romero 1, 27003 Lugo, A Coruña, Spain.
E-mail address: raymundoocaranza@yahoo.com (R. Ocaranza Sánchez).









