
A 66-year-old woman with severe functional tricuspid regurgitation and significant septal-anterior leaflet separation was admitted for transcatheter edge-to-edge repair. The patient’s prior informed consent was obtained for the intervention and subsequent publication of her case.
A chorda tendinea ruptured during the implantation of the first TriClip XTW system (Abbott Laboratories, United States) leading to a prolapsed severe anterior leaflet and increased valvular regurgitation (figure 1, video 1 of the supplementary data). Therefore, we decided to implant multiple devices in a “zip-like” sequence. We implanted the first device close to the anteroseptal commissure, followed by a second XTW device, which was deployed more medially. However, the septal leaflet detached after removing the blockade and prior to its release (figure 2A). Given the risk of embolization, we stabilized the system, kept it static, and eventually accessed the contralateral femoral vein with yet another TriClip XT system (Abbott Laboratories, United States) (figure 2B-D, videos 2 and 3 of the supplementary data). We implanted a third TriClip XT system over the septal-posterior leaflets and released the 2 systems. We completed the procedure with the implantation of a final TriClip XT system between the second and third devices, with satisfactory results (figure 3, video 4 of the supplementary data).
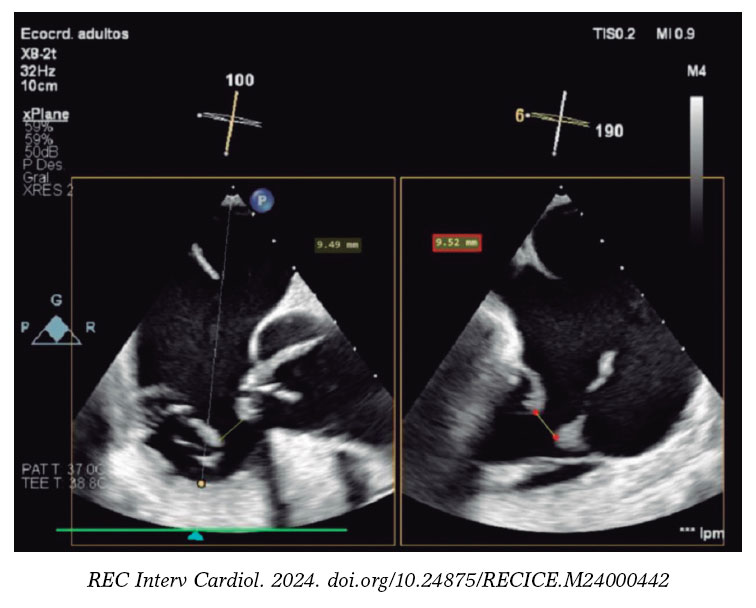
Figure 1.
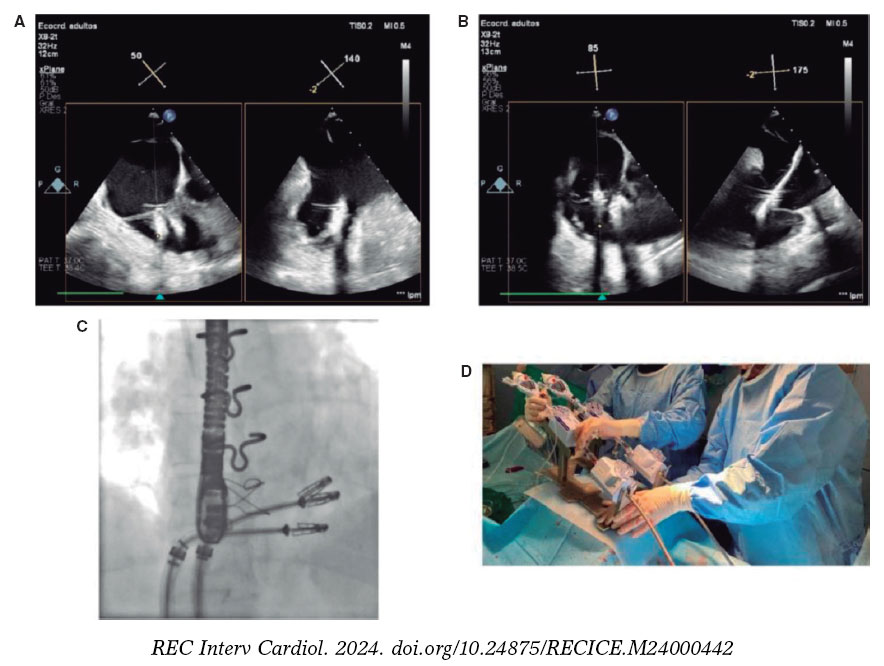
Figure 2.
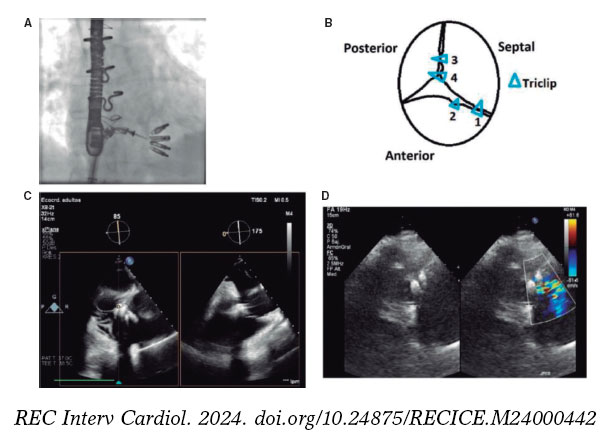
Figure 3.
The simultaneous deployment of 2 systems for tricuspid repair was a previously known strategy to solve large coaptation defects. Their use as a bailout technique is a feasible option to solve partial leaflet detachment. Morover, the combined use of transesophageal echocardiography and fluoroscopy, along with coordinated team effort between echocardiography experts and interventional cardiologists, is of paramount importance.
FUNDING
None declared.
ETHICAL CONSIDERATIONS
The present study did not require evaluation by the ethics committee. It represents a real-life case of a structural heart procedure routinely performed in our cath lab, with specific aspects of interest, particularly for interventional cardiologists performing this technique. The patient’s prior written informed consent was obtained to perform the procedure and publish the case.
STATEMENT ON THE USE OF ARTIFICIAL INTELLIGENCE
No artificial intelligence was used in the development of this article.
AUTHORS’ CONTRIBUTIONS
J.M. Hernández-García, and J. Alonso-Briales were directly involved in the procedure as interventional cardiologists. F. Carrasco-Chinchilla served as the echocardiography expert to guide the procedure. V.M. Becerra-Muñoz, and M. Luna-Morales contributed to the data curation process and drafted the manuscript with help from the other authors.
CONFLICTS OF INTEREST
F. Carrasco-Chinchilla, and J.M. Hernández-García have collaborated with Abbott Laboratories as proctors. The remaining authors declared no conflicts of interest whatsoever.
SUPPLEMENTARY DATA
Vídeo 1. Betanzos JL. DOI: 10.24875/RECICE.M24000442
Vídeo 2. Betanzos JL. DOI: 10.24875/RECICE.M24000442
Vídeo 3. Betanzos JL. DOI: 10.24875/RECICE.M24000442
Vídeo 4. Betanzos JL. DOI: 10.24875/RECICE.M24000442













