
A 51 year-old-male, with a diagnosis of severe pulmonary stenosis treated with surgical commissurotomy at the age of 4, was admitted due to severe right heart failure.
The echocardiography showed severe pulmonary regurgitation, severe right ventricular dilatation with moderate systolic dysfunction, severe tricuspid regurgitation with mild pulmonary hypertension. The magnetic resonance angiography showed pulmonary trunk dilatation. Surgery was ruled out due to high risk (morbid obesity, chronic dialysis).
A staged percutaneous procedure was planned, including pre-stenting with one XXL AndraStent premounted on a 30 mm balloon. After placing the stent embolized to the right pulmonary artery. Recovery was unsuccessful and a second stent had to be deployed (premounted on a 35 mm balloon). The pulmonary annulus size was 31 mm, so the direct implantation of a conventional valve (SAPIEN XT or Melody) was not recommended.
Several weeks later, a 22 mm Melody valve and a 37 mm long covered BeGraft stent premounted on a 12 mm balloon were simultaneously placed in parallel inside the stent and sequentially inflated (figure 1). Then a 16 mm AVP-2 device was placed inside the stent to occlude the lumen (figure 2 and figure 3). The final result was good, with mild pulmonary regurgitation (video 1 of the supplementary data). Follow-up at 16 months shows normal valve function and mild pulmonary regurgitation.
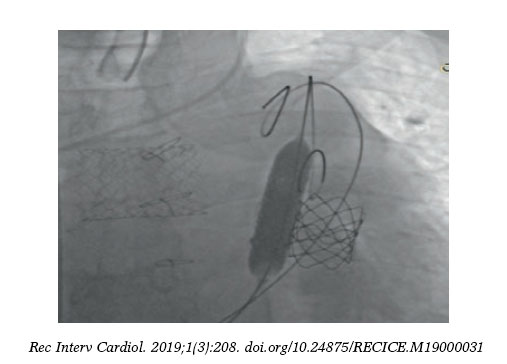
Figure 1
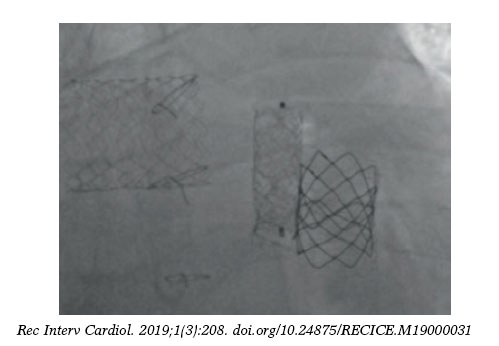
Figure 2
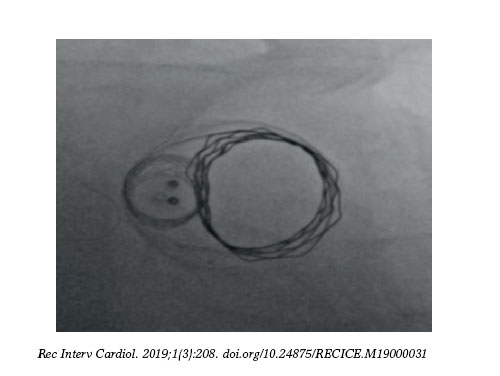
Figure 3
This hybrid technique with a covered stent and a Melody valve can be a safe alternative therapeutic option for patients with very large native right ventricle outflow tracts. These techniques should be reserved for patients with high surgical comorbidity.
SUPPLEMENTARY DATA
Video 1. Hernández F. DOI: 10.24875/RECICE.M19000031












