
The authors describe the case of a 67-year-old woman who presented initially with an anterior ST-segment elevation myocardial infarction. Emergency coronary angiography revealed the presence of 95% stenosis in the middle segment of the left anterior descending coronary artery (LAD), and 90% stenosis in the middle segment of the right coronary artery (RCA). Primary percutaneous coronary intervention (PCI) of the mid LAD was performed. Two weeks later, elective PCI of the mid RCA was performed: we advanced a hydrophilic guidewire towards the distal RCA, predilated the lesion with a 2.25 mm × 15 mm balloon, implanted a 3.0 mm × 38 mm zotarolimus-eluting stent, and postdilated with 2.75 mm × 12 mm and 2.5 mm × 8.0 mm balloons. Although the angioplasty was successful, we observed contained contrast extravasation in a posterolateral artery branch (figure 1A,B; video 1 of the supplementary data). Echocardiography revealed no significant pericardial effusion. Coronary angiography reassessment performed 3 days later documented an Ellis type 3 coronary perforation with an evident fistulous tract to the venous system (figure 2; video 2 of the supplementary data). We advanced an Excelsior SL-10 microcatheter (Stryker, United States) towards the proximal end of the fistula (figure 3A) and delivered a 2 mm × 4 cm coil, which successfully occluded the vessel (figure 3B). There were no complications during hospitalization or at the follow-up.
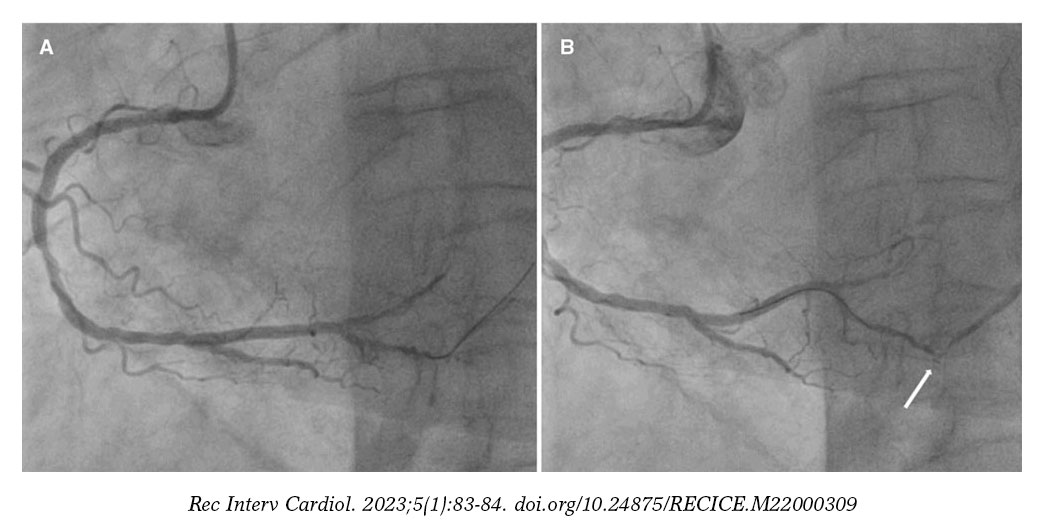
Figure 1.
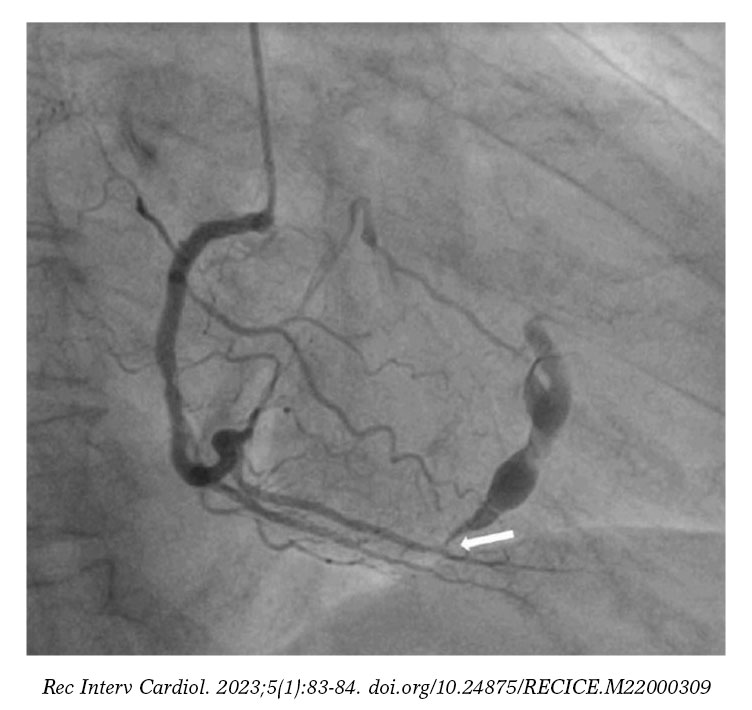
Figure 2.
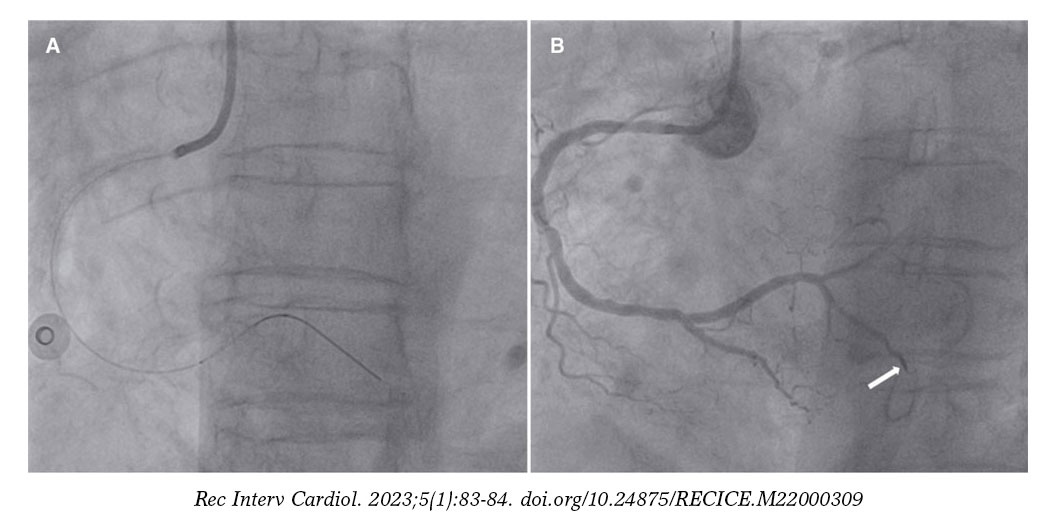
Figure 3.
Coronary artery perforation is a rare complication of PCI. Incidence rate is between 0.1% and 3.0%. Coronary perforations potentially result in severe complications like cardiac tamponade or arteriovenous fistula formation. Iatrogenic fistulae have a variable clinical course depending on the size and degree of left-to-right shunt. Treatment guidelines are not well established, and options reported include conservative, percutaneous or surgical management. Informed consent and authorization to publish these figures and videos were obtained from the patient.
FUNDING
None whatsoever.
AUTHORS’ CONTRIBUTIONS
P.D.A. Leite Medeiros was responsible for analyzing the case report and drafting the manuscript. J. Costa, and C. Galvão Braga performed the coronary intervention and reviewed both the manuscript and its figures. All authors approved the final version of the manuscript.
CONFLICTS OF INTEREST
The authors do not have any conflicts of interest.
SUPPLEMENTARY DATA
Vídeo 1. Araújo PD. DOI: 10.24875/RECICE.M22000309
Vídeo 2. Araújo PD. DOI: 10.24875/RECICE.M22000309












