
Cardiac allograft vasculopathy is characterized by the absence of lipid-rich plaques. However, transplant recipients may also develop lesions that resemble traditional atherosclerosis. Tacrolimus and everolimus, which are commonly used in transplant recipients, are associated to proatherogenic side effects such as hyperglycemia, hyperlipidemia and hypertension. Everolimus also triggers the release of several proinflammatory cytokines such as interleukin-6 and tumor necrosis factor α. Thus, inflammation, endothelial failure and hyperlipidemia are shared pathophysiological processes common to native in-stent neoatherosclerosis and transplant atherosclerosis.
We hereby present the case of a 50 year-old-male with a history of heart transplant 18 years ago with a zotarolimus-eluting stent implanted in his left anterior descending artery 16 months ago. The patient was administered immunosuppressive agents including quad- ruple therapy with corticosteroids, mycophenolate, tacrolimus and everolimus. The patient was admitted to the hospital due to acute heart failure. The coronary angiography conducted showed severe in-stent restenosis (figure 1A). The optical coherence tomography (OCT) showed the presence of early in-stent neoatherosclerosis with lipid-laden plaque similar to the morphological appearance so typical of native neoatherosclerosis (red asterisk) and vasa vasorum (green asterisk) (figure 1B, figure 1C). To avoid multiple metallic layers (red arrows), one bioresorbable vascular scaffold (green arrows) was deployed in-stent. The angiographic and OCT follow-up 1-month later confirmed the presence of scaffold patency with most struts uncovered (figure 2A, figure 2B, figure 2C). This is the first description of in-stent neoathero- sclerosis in a transplant recipient that occurred a few months after deploying the stent. Since the cardiac allograft vasculopathy is often silent and catastrophic, close metabolic control and invasive monitoring through images is advisable in these patients.
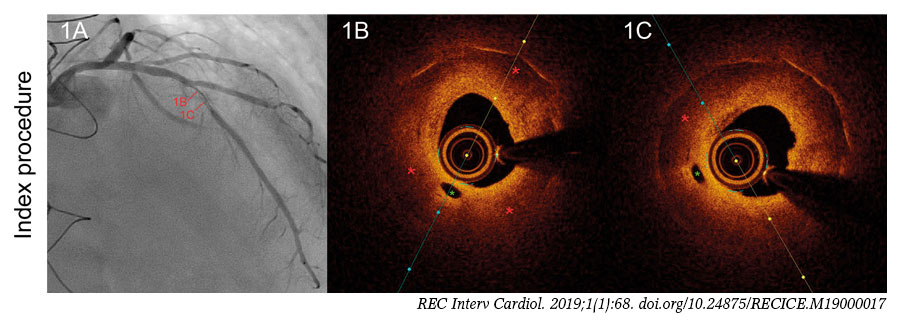
Figure 1.
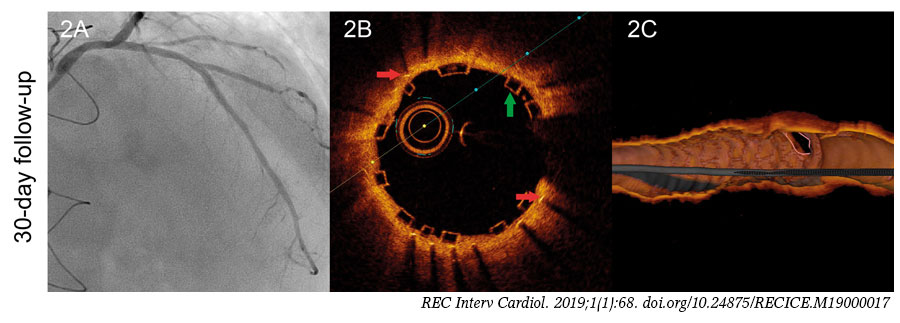
Figure 2.












