
The adoption of transcatheter tricuspid valve repair (TTVR) with the edge to edge technique has rapidly grown. Functional tricuspid regurgitation (TR) is the most common indication, and the most common approaches are to grasp either the septal and anterior (SL-AL) or septal and posterior leaflets (SL-PL).
A 78-year-old man presented with signs of right heart failure. Transesophageal echocardiography (TEE) revealed severe functional mitral regurgitation (MR) and torrential organic TR due to severe PL prolapse (figure 1A-C, arrows videos 1 and 2 of the supplementary data) in a tricuspid IIIA valve morphology (figure 1D, video 3 of the supplementary data). After heart team discussion, the patient was scheduled for TTVR.
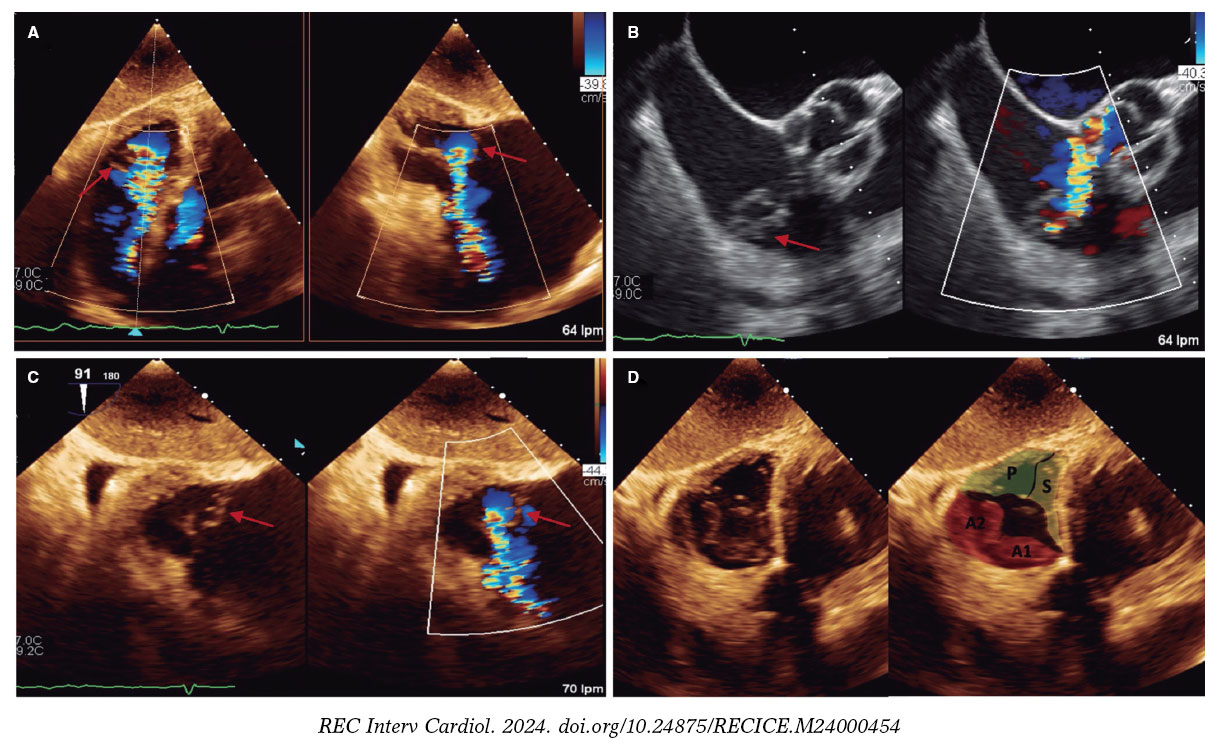
Figure 1.
After successful transcatheter mitral valve repair, TTVR was performed. Grasping both the tricuspid PL and SL did not significantly reduce the TR after several attempts. Consequently, to stabilize the posterior prolapse, we decided to perform a PL-AL grasping strategy. An XTW TriClip (Abbott Vascular, California, United States) was implanted between the PL and the A2 scallop, with a vertical orientation at the transgastric TEE view (figure 2A, video 4 of the supplementary data). Residual moderate TR from PL-SL coaptation was then observed (figure 2A, video 5 of the supplementary data). Therefore, a second XT TriClip oriented perpendicularly to the first device was aimed between the PL and SL (figure 2B). A triple-orifice tricuspid valve result showed trace residual TR and no significant stenosis, with a mean gradient of 1 mmHg (figure 2, videos 6 and 7 of the supplementary data). At 3 months of follow-up, residual TR was trivial (video 8 of the supplementary data) and the patient remained symptom free. In certain scenarios like this, an alternative strategy such as PL-AL grasping using TG X-Plane views could be a useful approach.
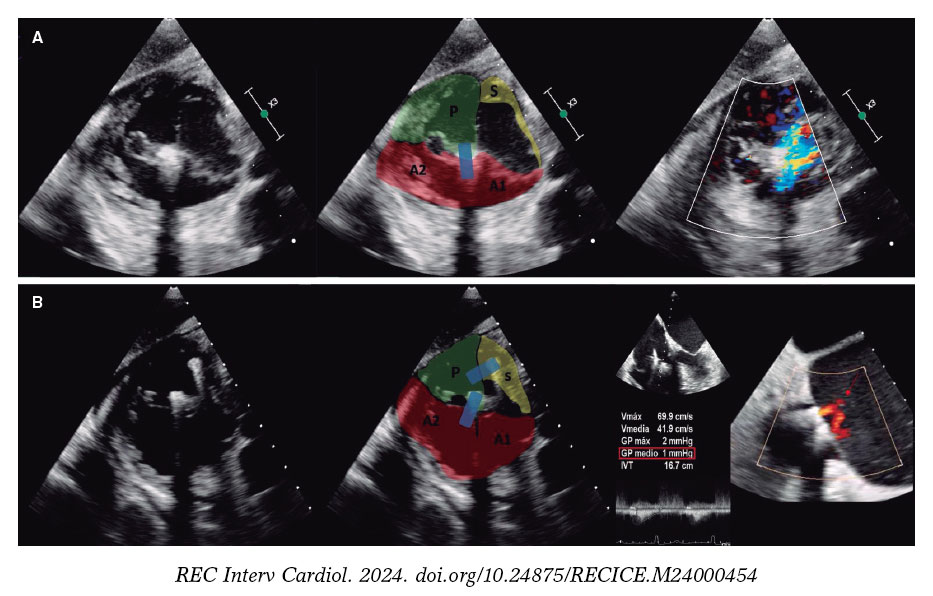
Figure 2.
FUNDING
No funding was received for the development of this manuscript.
ETHICAL CONSIDERATIONS
The authors of this article confirm that written consent was obtained and archived.
STATEMENT ON THE USE OF ARTIFICIAL INTELLIGENCE
No artificial intelligence was used in the preparation of this manuscript.
AUTHORS’ CONTRIBUTIONS
J.L. Betanzos, A. Alperi, V. León, I. Silva, and I. Pascual participated in the writing, critical review, and final approval of the manuscript. J.L. Betanzos and A. Alperi contributed equally. P. Avanzas participated in the critical review and final approval of the manuscript.
CONFLICTS OF INTEREST
The authors have no conflicts of interest to report.
SUPPLEMENTARY DATA
Vídeo 1. Betanzos JL. DOI: 10.24875/RECICE.M24000454
Vídeo 2. Betanzos JL. DOI: 10.24875/RECICE.M24000454
Vídeo 3. Betanzos JL. DOI: 10.24875/RECICE.M24000454
Vídeo 4. Betanzos JL. DOI: 10.24875/RECICE.M24000454
Vídeo 5. Betanzos JL. DOI: 10.24875/RECICE.M24000454
Vídeo 6. Betanzos JL. DOI: 10.24875/RECICE.M24000454
Vídeo 7. Betanzos JL. DOI: 10.24875/RECICE.M24000454
Vídeo 8. Betanzos JL. DOI: 10.24875/RECICE.M24000454










