
This is the case of a 78-year-old man with revascularized coronary artery disease 10 years ago (left anterior descending coronary artery and left circumflex artery) who was admitted to the hospital with signs of ST-segment elevation acute coronary syndrome. The angiography shows an unusual image on the proximal left anterior descending coronary artery that seems to be causing an angiographically significant stenosis (figure 1A,B). To confirm diagnosis, a catheter is unsuccessfully advanced with optical coherence tomography (OCT) guidance through a polymeric guidewire while trying to cross the most stenotic region. Two attempts are made after predilatation (with balloons of 1.5 mm and 2.5 mm in diameter) that prove unsuccessful. Afterwards, a guide catheter extension system is advanced (figure 1D) that successfully crosses the lesion facilitating the OCT that reveals the presence of an underexpanded coronary stent with complete endothelization, and a possible thrombus attached to it (figure 1C). Upon suspicion that this is the culprit lesion, decision is made to treat it. To crush the underexpanded stent against the lumen of the vessel, it is first effortlessly predilated using a 3.5 mm x 12 mm balloon. Afterwards, a 3.5 mm x 15 mm drug-eluting stent is implanted with good angiographic results (figure 1E). A new OCT confirms the excellent expansion of the new stent including the entire forgotten stent that is crushed between the new stent and the vessel endothelium (figure 1F).
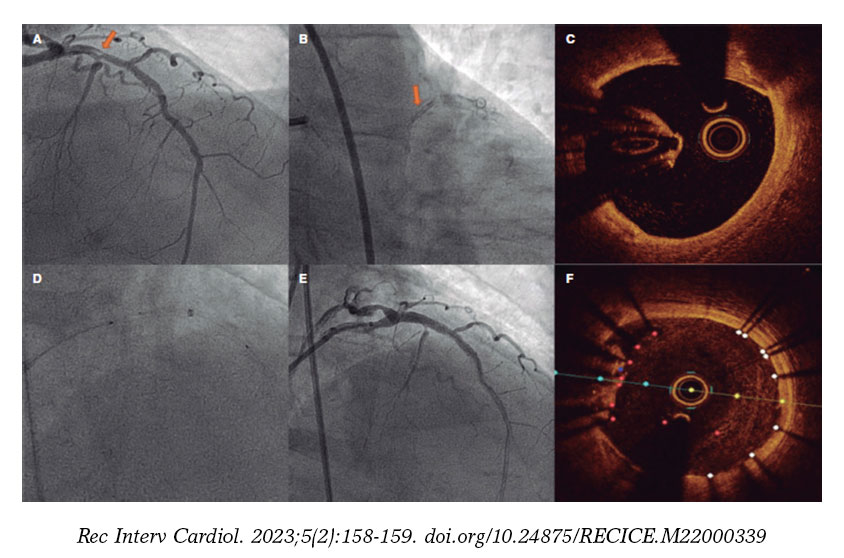
Figure 1.
Stent loss inside the coronary tree is a rare complication that can, however, be solved if removed during the procedure. However, when forgotten for years, the stent endothelizes and its extraction becomes complicated and is no stranger to complications. In these cases, the most efficient option is to exclude it by implanting a new drug-eluting stent.
The patient’s written informed consent was requested before publishing this article.
FUNDING
None whatsoever.
AUTHORS’ CONTRIBUTIONS
All the authors were involved in the procedure. They also reviewed the images and drafted the manuscript.
CONFLICTS OF INTEREST
R. Moreno in an associate editor of REC: Interventional Cardiology; the journal’s editorial procedure to ensure impartial handling of the manuscript has been followed.











