
Seventy-four-year-old male patient admitted with non-ST-elevation acute myocardial infarction. The coronary angiography performed revealed the presence of right coronary artery stenosis with a giant coronary artery aneurysm (CAA) and high thrombus burden (figure 1A). Dual antiplatelet and anticoagulation therapies were recommended for its exclusion in a staged procedure. After confirmation of thrombus reduction (figure 1B), predilatation was attempted and both the length of the CAA (40 mm) and the landing zone were measured on the intravascular ultrasound (IVUS) (figure 1C). From proximal to distal, two 5 mm x 26 mm-PK-Papyrus covered coronary stents (PCS) (Biotronik, Switzerland) were deployed. The overlapping stent zone was confirmed using the StentBoost imaging modality (Philips Medical Systems, Nederland) (figure 1D) and the stent was deployed under fluoroscopic guidance in the absence of any respiratory movements. The subsequent angiography performed revealed an incomplete CAA exclusion (figure 1E) despite postdilatation with a 5.5 mm noncompliant balloon (NCB). The IVUS confirmed the existence of a gap between both stents due to stent shortening (E2, figure 1E and video 1 of the supplementary data). Another 5 mm × 15 mm PCS was deployed followed by postdilatation with a 5.5 mm NCB. Both the angiography and the IVUS confirmed the complete CAA exclusion (figure 1F and video 2 of the supplementary data). Patient has given his verbal consent for publication of this case report.
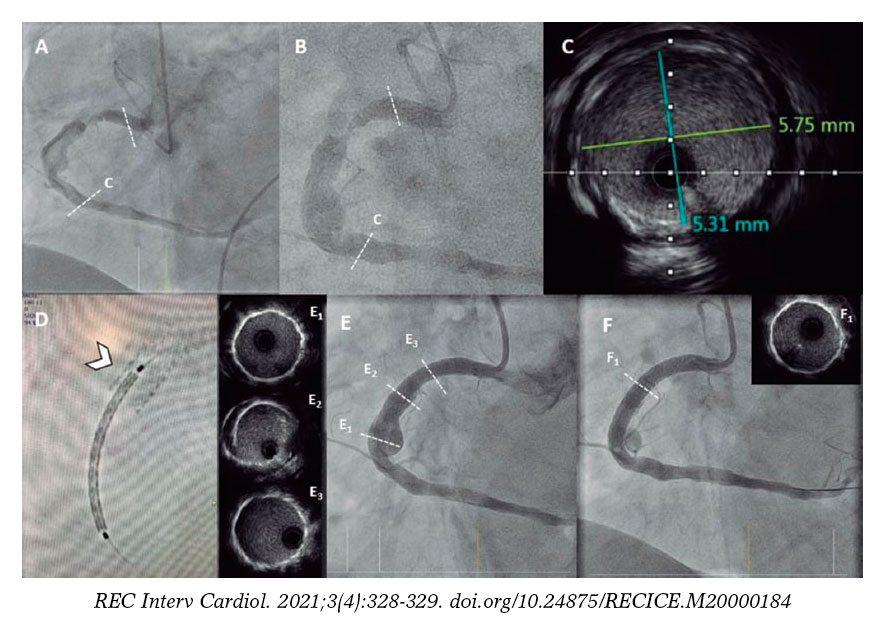
Figura 1.
The management of CAAs is still controversial. PCSs designed to treat coronary perforations have also been used to treat CAA exclusions. We described how the significant shortening of these devices, especially when using larger diameters, can cause incomplete CAA exclusion (or perforation). Also, that intracoronary imaging modalities are essential for optimization purposes. As far as we know, this is the first description ever of a Papyrus stent shortening combining angiography, IVUS, and StentBoost.
FUNDING
No funding was received for this work.
AUTHORS' CONTRIBUTIONS
Each person listed as an author has participated to: a) Conceive, plan and perform the work leading to the report. b) Write the report or reviewed successive versions. c) Approve the final version.
CONFLICTS OF INTEREST
R. Moreno is associate editor of REC: Interventional Cardiology. The journal’s editorial procedure to ensure impartial handling of the manuscript has been followed.
SUPPLEMENTARY DATA
Vídeo 1. Gonzálvez-García A. DOI: 10.24875/RECICE.M20000184
Vídeo 2. Gonzálvez-García A. DOI: 10.24875/RECICE.M20000184
Corresponding author: Hospital Universitario La Paz, Paseo de la Castellana 261, 28046 Madrid, Spain.
E-mail address: arianagonzalvez@gmail.com (A. Gonzálvez-García).










