
This is the case of a 55-pound 6-year-old male diagnosed with right coronary artery (RCA) fistula draining into the right ventricle (RV). Due to progressive dilatation of the RCA, percutaneous closure was decided.
The femoral artery and veins were canalized using 5-Fr and 6-Fr introducer sheaths, respectively. A right coronary angiography revealed the presence of a RCA proximal to the 7.1 mm fistula—a fistula with a 11.2 mm × 7.2 mm bilobulated aneurysm with a 2.1 mm right ventricular outflow tract—and a coronary artery distal to the fistula of normal diameter (figure 1, figure 2, and video 1 of the supplementary data).
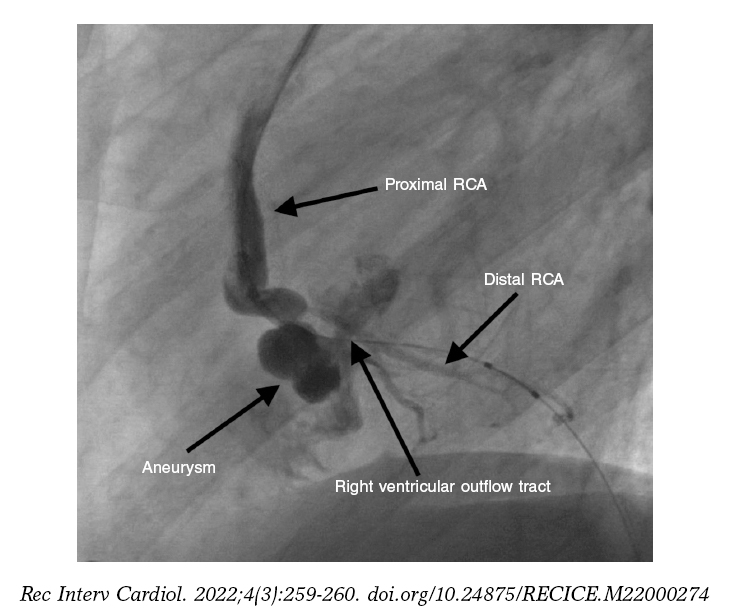
Figure 1.
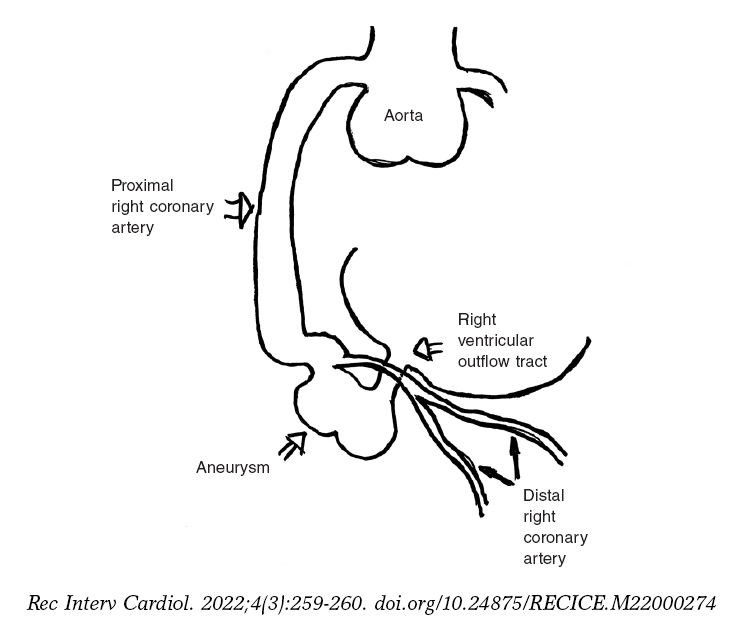
Figure 2.
The fistula was catheterized with a coronary guidewire that was advanced towards the pulmonary artery where it was captured with a snare creating an arteriouvenous loop. From the venous side of this loop a 4 mm × 8 mm Apex Monorail balloon catheter (Boston Scientific, United States) was advanced and then inflated in the ostium of the fistula in the RV for 10 minutes without any signs of ischemia.
Considering the risk of progressive aneurysmal dilatation if the fistula was closed in its distal edge and given the lack of space to fit a device in its proximal edge, it was decided to embolize the aneurysm using microcoils. Using a 5-Fr JR4 guide catheter allocated in the RCA an Excelsior SL microcatheter (Stryker Neurovascular, United States) was advanced. The aneurysm was embolized with 6 Barricade microcoils (Invine, United States) that were released after confirming their stable position inside the aneurysm and lack of residual shunt (figure 3 and video 2 of the supplementary data). No complications were reported after cardiac catheterization. The patient’s father gave his consent to publish the case.
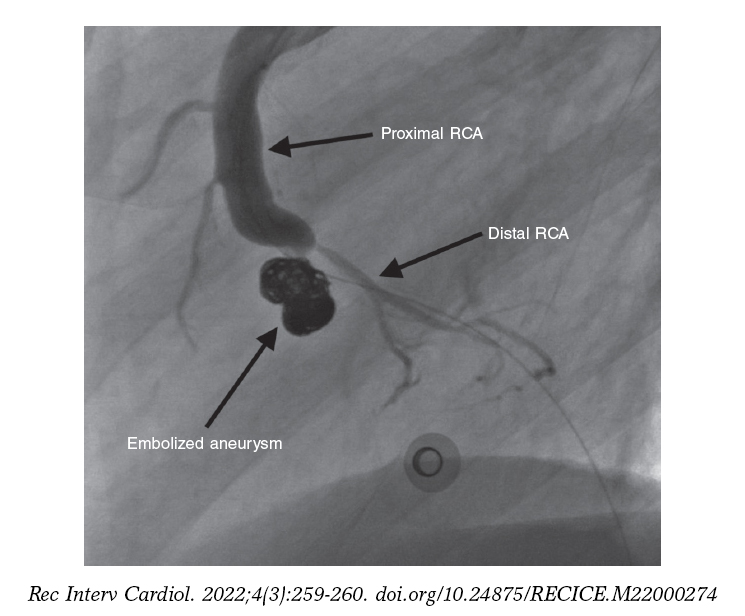
Figure 3.
FUNDING
None whasoever.
AUTHORS’ CONTRIBUTIONS
A. Mendoza drafted the manuscript. D. Herrera, M. Flores, J. Campollo, and F. Ballenilla participated in case resolution, and in the revision, and final approval of this manuscript.
CONFLICTS OF INTEREST
None reported.
SUPPLEMENTARY DATA
Vídeo 1. Mendoza A. DOI: 10.24875/5/RECICE.M22000274
Vídeo 2. Mendoza A. DOI: 10.24875/5/RECICE.M22000274
* Corresponding author:
E-mail address: alberto.mendoza@salud.madrid.org (A. Mendoza).









