
This is the case of a 77-year-old woman with hypertension, dyslipidemia, and stage V chronic kidney disease. While on hemodialysis she experiences precordial pain due to paroxysmal atrial fibrillation with rapid ventricular response. The electrocardiogram shows widespread ST-segment depression. The blood tests confirm the presence of slightly elevated ultrasensitive troponin I levels later showing an ascending and descending curve suggestive of acute coronary syndrome. A coronary angiography is indicated after these findings.
The coronary angiography shows a single right coronary artery (figure 1) running through the atrioventricular sulcus and generating branches with perfusion to all myocardial territories of the left and right ventricles (figure 2 and video of the supplementary data).
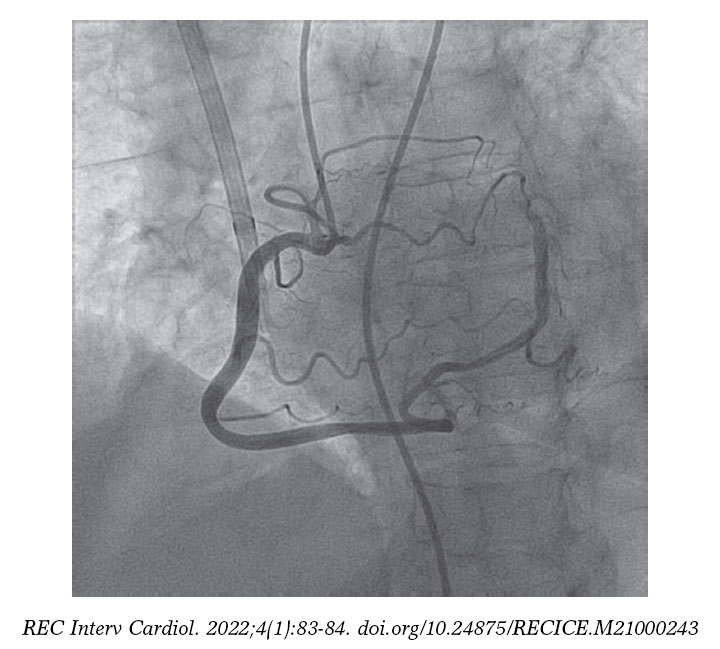
Figure 1.
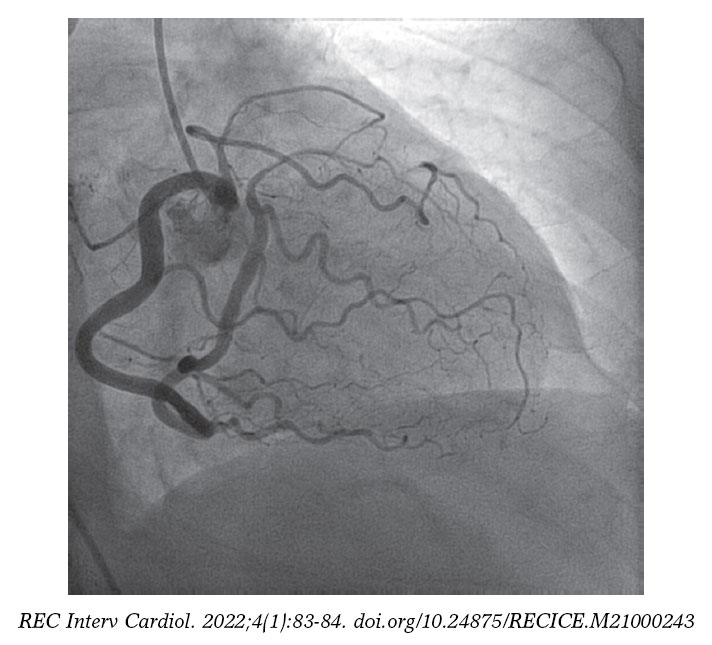
Figure 2.
The prevalence of single right coronary artery is between 0.024% and 0.066%; the single right coronary artery is, actually, one of the rarest variants.
In these patients, flow runs through a system with a large sequence of serial resistances. Based on these findings, we could argue that the perfusion of medioapical segments would be in a situation of «relative» ischemia compared to the rest. This would exacerbate in situations of greater myocardial demand as in tachyarrhythmias.
Although cases of chest pain or angina have been reported in patients with this anomaly who did not have coronary atherosclerosis, it is difficult to establish a causal correlation between the angiographic finding and the clinical signs. Coronary microcirculation was not assessed either, which is why the pathophysiological mechanism suggested is pure speculation.
The patient’s written informed consent was obtained before publishing her case.
FUNDING
None whatsoever.
AUTHORS’ CONTRIBUTIONS
C. Garilleti, and J. M de la Torre-Hernández drafted the manuscript. A. Gil Ongay conducted the critical review of its content and gave his final approval.
CONFLICTS OF INTEREST
J. M de la Torre-Hernández is the editor-in-chief of REC: Interventional Cardiology; the journal’s editorial procedure to ensure impartial handling of the manuscript has been followed. The remaining authors declared no conflicts of interest whatsoever.
SUPPLEMENTARY DATA
Vídeo 1. Garilleti Cámara C. DOI: 10.24875/RECICE.M21000243
* Corresponding author: Magallanes 40-42 2 C, 39007 Santander, Cantabria, Spain.
E-mail address: celia.garilleti@scsalud.es (C. Garilleti Cámara).









