
Sixty-six-year-old male patient with a past medical history of mitral and aortic valve replacement in 1983. Back in 2005 he underwent a new aortic valve replacement due to prosthetic valve dysfunction. In 2018, also due to prosthetic valve dysfunction, a new mitral valve replacement was performed with a size 27 Bicarbon Fitline heart valve (Sorin Group, Italy).
Three months later the patient was hospitalized with functional class III-IV heart failure according to the New York Heart Association (NYHA) and hemolytic anemia with multiple mitral paravalvular leaks quantified as severe regurgitation. In a single medical-surgical session it was decided to perform percutaneous treatment due to the patient’s high surgical risk. The percutaneous closure of the leaks was performed using 7 Amplatzer Vascular Plug III devices (figure 1E) that resulted in minimal residual leaks.
In 2019 the patient presented with NYHA functional class III-IV and hemolytic anemia back again. The 3D echocardiogram performed revealed the presence of 2 severe mitral paravalvular leaks (figure 2A,B) (video 1 of the supplementary data). Percutaneous approach was attempted. An antegrade venoarterial circuit via transseptal puncture was built using a 0.035 in hydrophilic guidewire (figure 1A,B) (videos 2 and 3 of the supplementary data), 2 12/5 mm Amplatzer Vascular Plug III devices were implanted (figure 1C) (videos 4 and 5 of the supplementary data), and 9 devices of the same type surrounding the prosthetic circumference (figure 1D and figure 2D) (video 6 of the supplementary data). The procedure was completed uneventfully. The transesophageal echocardiography performed during the procedure confirmed the reduction of mitral paravalvular leaks now quantified as mild regurgitation (figure 2C) (video 7 of the supplementary data). Disease progression was good, and the patient was discharged with NYHA functional class II-III, corrected anemia (hemoglobin of 12 g/dL), and outpatient follow-up.
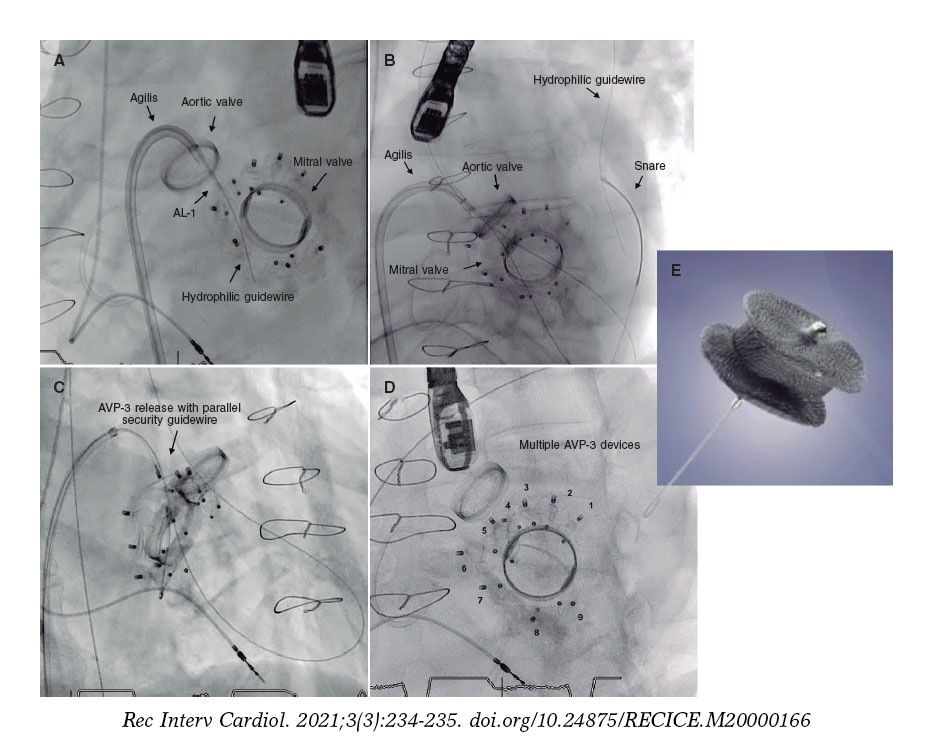
Figure 1.
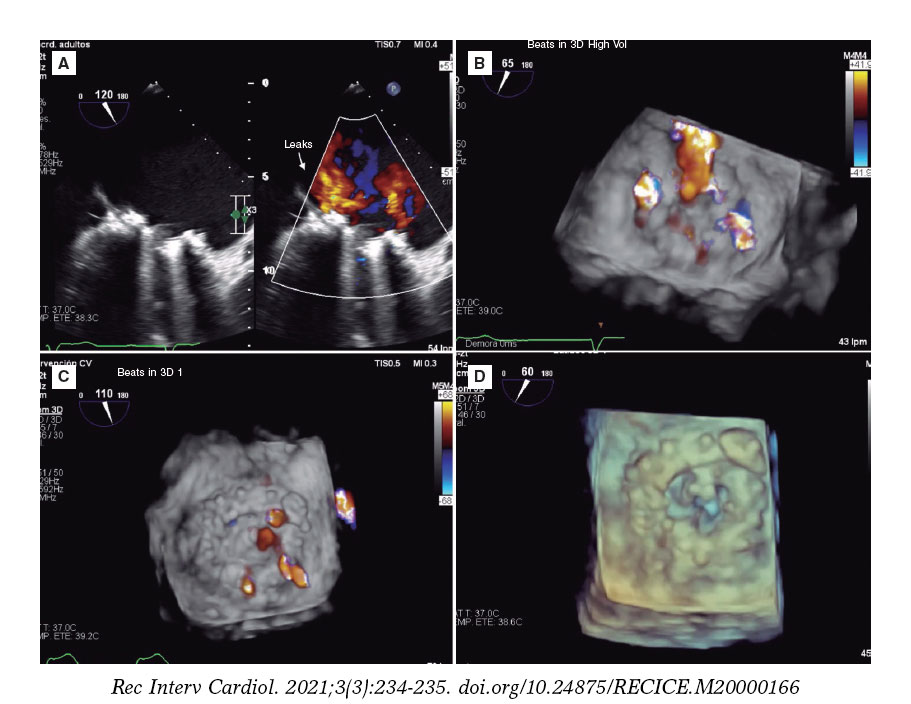
Figure 2.
CONFLICTS OF INTEREST
I. Cruz Gónzalez is proctor for Abbott.
SUPPLEMENTARY DATA
Video 1. Gómez Silva M. DOI: 10.24875/RECICE.M20000166.
Video 2. Gómez Silva M. DOI: 10.24875/RECICE.M20000166.
Video 3. Gómez Silva M. DOI: 10.24875/RECICE.M20000166.
Video 4. Gómez Silva M. DOI: 10.24875/RECICE.M20000166.
Video 5. Gómez Silva M. DOI: 10.24875/RECICE.M20000166.
Video 6. Gómez Silva M. DOI: 10.24875/RECICE.M20000166.
Video 7. Gómez Silva M. DOI: 10.24875/RECICE.M20000166.
* Corresponding author: Unidad de Hemodinámica, Hospital Dr. Gustavo Fricke, Avda. Álvarez 1532, Viña del Mar, Valparaíso, Chile.
E-mail address: marceloalejandro.gomezsilva@gmail.com (M. Gómez Silva).









