
Seven-year-old male with single ventricle in the postoperative of a fenestrated extracardiac Fontan procedure. The echocardiography performed 7 days after the procedure confirmed the presence of a 20 mm pedunculated thrombus attached to the wall of the inferior vena cava (video 1 of the supplementary data).
Due to the risk of systemic embolism through the Fontan fenestration, the percutaneous extraction of the thrombus was attempted using an Amplatzer Vascular Plug II (AVP II) device (Abbott, United States).
A 6-Fr introducer sheath and a 10-Fr sheath were used for the catheterization of the right jugular vein and right femoral vein, respectively. The fenestration was found in the Fontan conduit using an angiography (figure 1). It was catheterized via jugular access and occluded by inflating the balloon of a 6-Fr Wedge-Pressure Catheter (Arrow, United States) to protect an eventual paradoxical embolism (figure 2). The transesophageal echocardiography performed revealed the location of the thrombus in the inferior vena cava and the diameter of the cava was measured at that level (15 mm). The introducer sheath was advanced via femoral access until it landed right underneath the insertion of the thrombus. Through this sheath a folded 16 mm AVP II device was advanced inside an 8-Fr multipurpose catheter that was advanced until it passed the thrombus distal edge. The AVP II was unfolded in this position and pulled back until it was finally inserted into the sheath located in the inferior vena cava (figure 3 and videos 2, 3, and 4 of the supplementary data). Although the thrombus was never retrieved, it disappeared leaving no trace of pulmonary embolism. The consent of the patient’s father was obtained for the publication of the case.
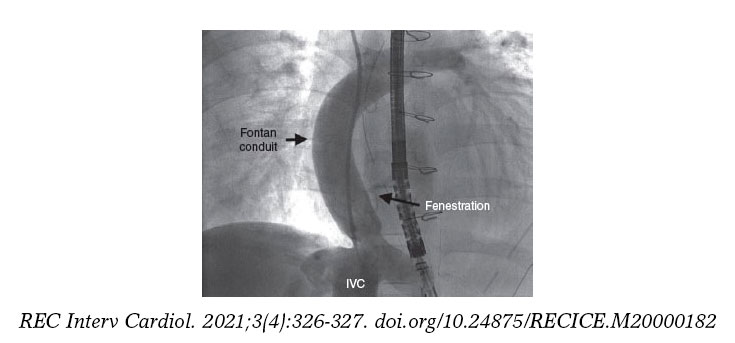
Figure 1.
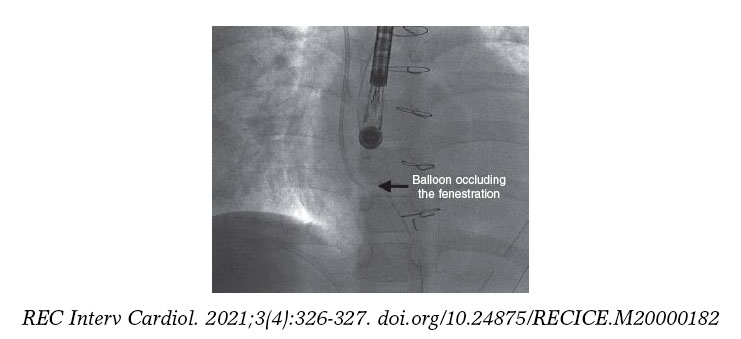
Figure 2.
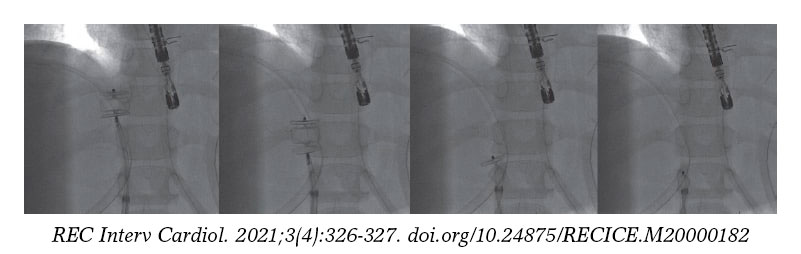
Figure 3.
FUNDING
None.
AUTHORS' CONTRIBUTIONS
All the authors have participated in the writing of this article and have read and approved the final version.
CONFLICTS OF INTEREST
None.
SUPPLEMENTARY DATA
Vídeo 1. Mendoza A. DOI: 10.24875/RECICE.M20000182
Vídeo 2. Mendoza A. DOI: 10.24875/RECICE.M20000182
Vídeo 3. Mendoza A. DOI: 10.24875/RECICE.M20000182
Vídeo 4. Mendoza A. DOI: 10.24875/RECICE.M20000182
Corresponding author: Instituto Pediátrico del Corazón, Hospital Universitario 12 de Octubre, Avda. de Córdoba s/n, 28041 Madrid, Spain.
E-mail address: alberto.mendoza@salud.madrid.org (A. Mendoza).









