
To the Editor,
Coronary occlusion is a more common complication after transcatheter aortic valve-in-valve implantation than after transcatheter aortic valve implantation over the native valve. It is due to the displacement of the veil of the surgical valve prior to transcatheter aortic valve implantation until occluding the coronary ostium.1 The risk is higher with surgical prostheses without stent and with those with veils mounted outside the stent. It also depends on the height of coronary ostia and width of sinuses.2
Coronary arteries can be protected by advancing a guidewire or even a stent inside the coronary artery at risk, which creates some sort of chimney to keep the ostium open3 with unpredictable results especially in the long-term.
Recently, the BASILICA technique (Bioprosthetic or native aortic scallop intentional laceration to prevent iatrogenic coronary artery obstruction) has been described to avoid coronary occlusions. It consists of lacerating the veil of the surgical prosthesis facing the ostium at risk with an electrified guidewire so that it opens when implanting the new prosthesis while leaving the ostium uncovered.4
This is the case of an 89-year-old woman—carrier of a 19 mm Mitroflow bioprosthesis (Sorin Group Inc., Mitroflow Division; Vancouver, Canada) due to severe aortic stenosis since 2010—who was admitted to our center due to heart failure. The echocardiogram confirmed the presence of severe aortic stenosis again due to valve degeneration. The internal area of the aortic annulus according to the coronary computed tomography angiography performed was 230 cm2 with a 54 mm-perimeter. Coronary arteries originated at the annulus 4 mm to the left and 9 mm to the right and with a 3.5 mm and 4.7 mm distance from the valve virtually implanted to the left and right ostia, respectively.
Given the risk of occlusion of the left coronary ostium, it was decided to approach this case using the valve-in-valve technique with a 23 mm Evolut PRO valve (Medtronic, Minneapolis, Minnesota, United States) using the BASILICA technique with fluoroscopy and transesophageal echocardiography guidance. Thus, via left femoral artery a 23 mm snare was advanced through a 6-Fr multipurpose catheter that crossed the bioprosthesis and allocated in the left ventricular outflow tract. Through this same artery a 0.18 inches pre-shaped guidewire was inserted, in parallel, that remained on the left ventricular apex to stabilize the position of the snare as shown on figure 1. A 14-Fr introducer sheath was used via right femoral artery (after valve implantation) to advance the system to perforate and then tear the veil. This system consisted of a 6-Fr AL 3 guide catheter with a 5-Fr 125 cm internal mammary diagnostic catheter and a 150 cm FINECROSS microcatheter (Terumo, Japan) with an ASAHI Astato guidewire. The whole process used a telescopic method.
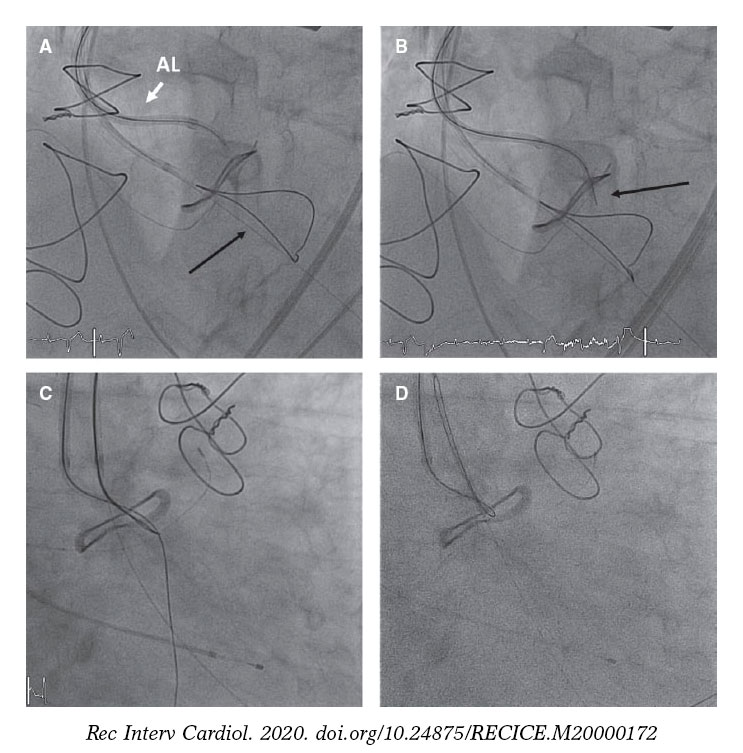
Figure 1. A: AL 3 guide catheter at the base of the left coronary veil of the Mitroflow bioprosthesis with a slightly protruding internal mammary diagnostic catheter. The radiopaque tip of the FINECROSS microcatheter and the Astato guidewire inside the internal mammary catheter can be seen. Snare positioned in the left ventricular outflow tract (arrow). B: Astato guidewire already in place in the left ventricle (arrow). C: guidrewire captured with the snare. D: Astato guidewire inserted into the multipurpose catheter with complete circuit.
After checking the exact position of the system before perforation on the frontal and lateral projections, the Astato guidewire external border (Asahi, Aichi, Japan) was connected to a 50-Watt electric scalpel. The guidewire—previously peeled with a scalpel blade—was advanced to the left ventricular outflow tract (figure 1). Afterwards, the guidewire was captured using the snare and the circuit was closed. Afterwards, the internal mammary catheter and the microcatheter were retrieved exposing the body of the Astato guidewire to be able to peel a short segment of it to later bend it in V-shape. This V-shape was advanced until the base of the veil that needed to be torn. Then, a high-support guidewire was advanced towards the LV by the 14-Fr introducer via right femoral artery, parallel to the snare, with the prosthesis ready to be implanted. Then the Astato guidewire was connected to the electrical scalpel, and a 70-Watt current was applied. Afterwards, the 2 borders of the circuit were removed to tear the veil.
In our case, after capturing the guidewire with the snare and while the V-shape was being prepared, the patient experienced severe hypotension with both aortic and mitral regurgitation, both severe. Since the transesophageal echocardiography confirmed that the patient was unresponsive to inotropic drugs, external cardiac massage was required that triggered the use of the BASILICA technique and valve implantation under cardiac massage (figure 2). After the implant, the patient stabilized. Compromise of coronary ostium was discarded and a significant aortic gradient was seen (mean gradient, 53 mmHg). Then, it was decided to proceed with postdilatation and fracture the prosthesis with a 20 mm noncompliant ATLAS balloon (BARD Medical, United States) with disappearance of residual gradient (residual 7 mmHg)
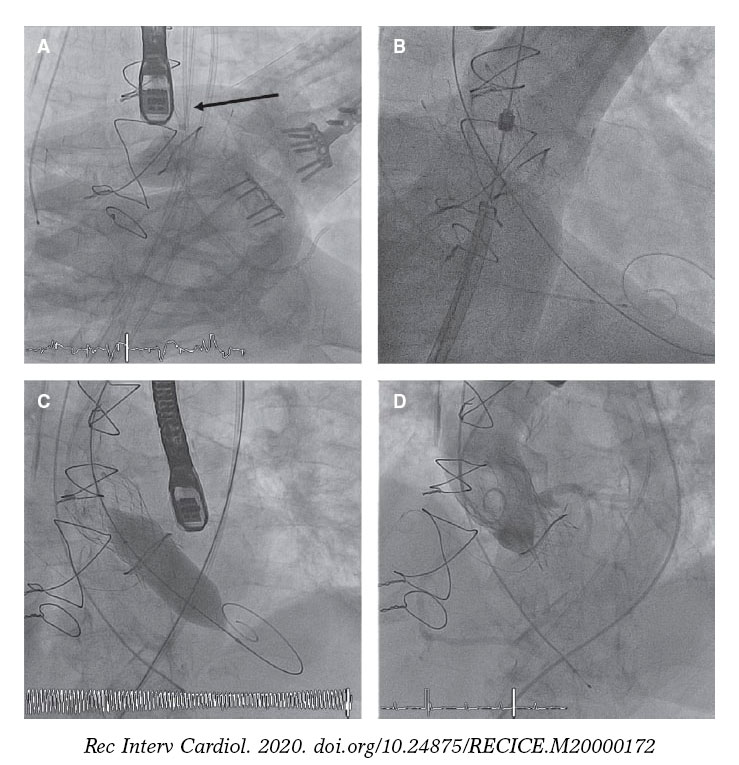
Figure 2. A: tear of the veil (BASILICA technique) under cardiac massage. The arrow points at the 2 catheters facing each other with the V-shaped Astato guidewire. B: Evolut PRO valve implantation under cardiac massage. C: dilatation with ATLAS balloon for fracture purposes. D: final aortography.
Disease progression was good, and the patient was discharged from the hospital after 9 days and following the implantation of a pacemaker due to complete AV block without other complications. She gave oral consent for the publication of the case.
The BASILICA technique is an effective alternative to avoid coronary occlusions and valve-in-valve procedures with high risk of occlusion. However, it is a demanding complex procedure with complications, that requires prior training. The snare can interfere with the mitral valve and cause regurgitation. Also, the tension of the circuit can cause severe aortic regurgitation with hemodynamic collapse.
FUNDING
No funding was received for this work.
AUTHORS' CONTRIBUTIONS
A. Albarrán González-Trevilla participated in the drafting and correction of the manuscript and in the performance of the procedure. J. García Tejada participated in the drafting of the manuscript. F. Sarnago Cebada participated in the correction of the manuscript. J. A. García Robles provided the echocardiogram images and participated in the procedure. M. Velázquez Martín participated in the correction of the manuscript. D. Dvir participated in the correction of the manuscript and the performance of the procedure.
CONFLICTS OF INTEREST
Nothing to declare.
REFERENCES
1. Holmes DR Jr, Nishimura RA, Grover FL, et al. STS/ACC TVT Registry. Annual Outcomes With Transcatheter Valve Therapy:From the STS/ACC TVT Registry. J Am Coll Cardiol. 2015;66:2813-2823.
2. Ribeiro HB, Rodés Cabau J, Blanke P, et al. Incidence, predictors, and clinical outcomes of coronary obstruction following transcatheter aortic valve replacement for degenerative bioprosthetic surgical valves:insights from the VIVID registry. Eur Heart J. 2018;39:687-695.
3. Abramowitz Y, Chakravarty T, Jilaihawi H, et al. Clinical impact of coronary protection during transcatheter aortic valve implantation:first reported series of patients. EuroIntervention. 2015;11:572-581.
4. Khan JM, Dvir D, Greenbaum AB, et al. Transcatheter laceration of aortic leaflets to prevent coronary obstruction during transcatheter aortic valve replacement. Concept to first-in-human. JACC Cardiovasc Interv. 2018;11:677-689.
Corresponding author: Cartagena 6, 2º D, 28028 Madrid, Spain.
E-mail address: agustin.albarrang@hotmail.com (A. Albarrán González-Trevilla).









