
Two-month baby recently treated with closure of perimembranous interventricular communication with congestive clinical signs in the postoperative period and echocardiographic suspicion of possible right coronary artery-to-right ventricle fistula confirmed on the cardiac computed tomography and catheterization with nonselective coronary angiography. Parents' informed consent was obtained for the dissemination of the case. A large coronary fistula—eligible for percutaneous closure—can be seen exiting the right coronary artery marginal branch and entering the right ventricular cavity with great dilatation of the right coronary artery proximal segment (figure 1). A 4-Fr carrier catheter is inserted into the right coronary artery and a guidewire is advanced towards the right ventricle. Assisted by an angioplasty balloon, the carrier catheter is then advanced towards the fistula proximal zone where eventually a 4 × 6 Amplatzer Vascular Plug (AVP4) device (Abbott, United States) is delivered resulting in the total occlusion of the defect with no interference with the distal right coronary artery (figure 2).
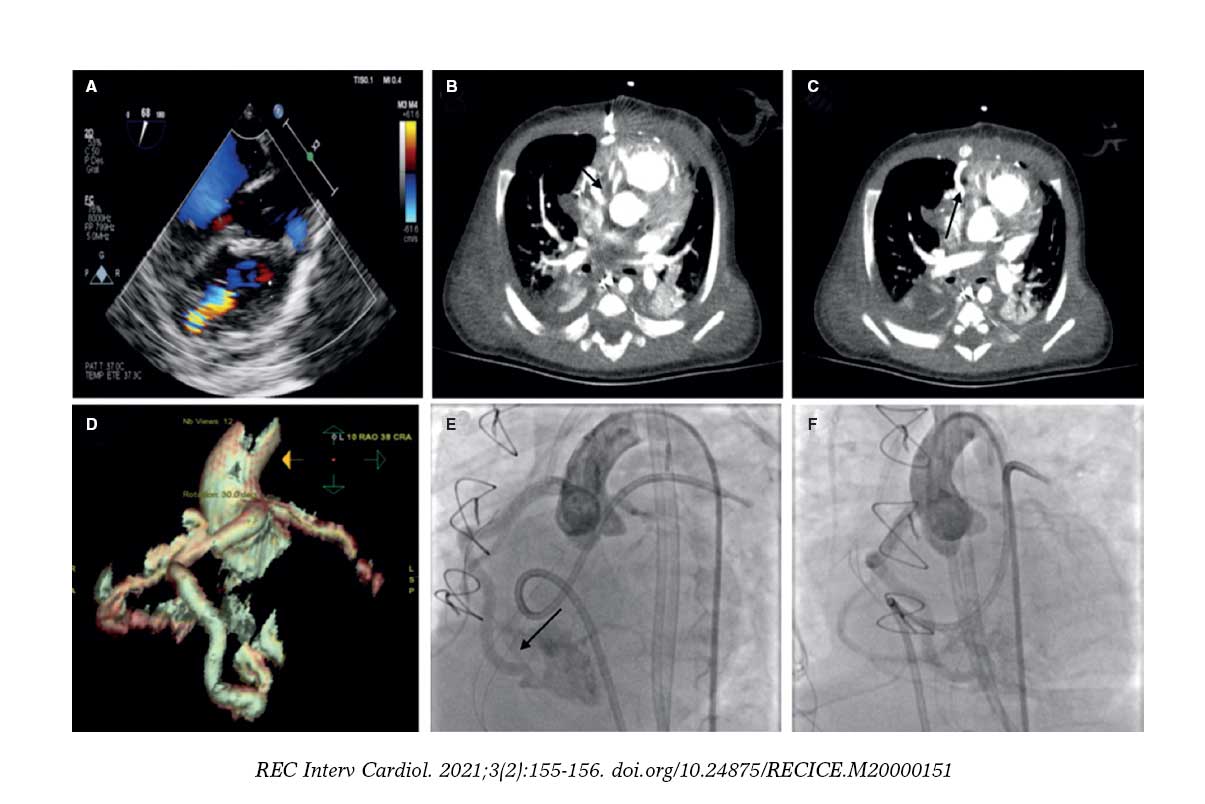
Figure 1.
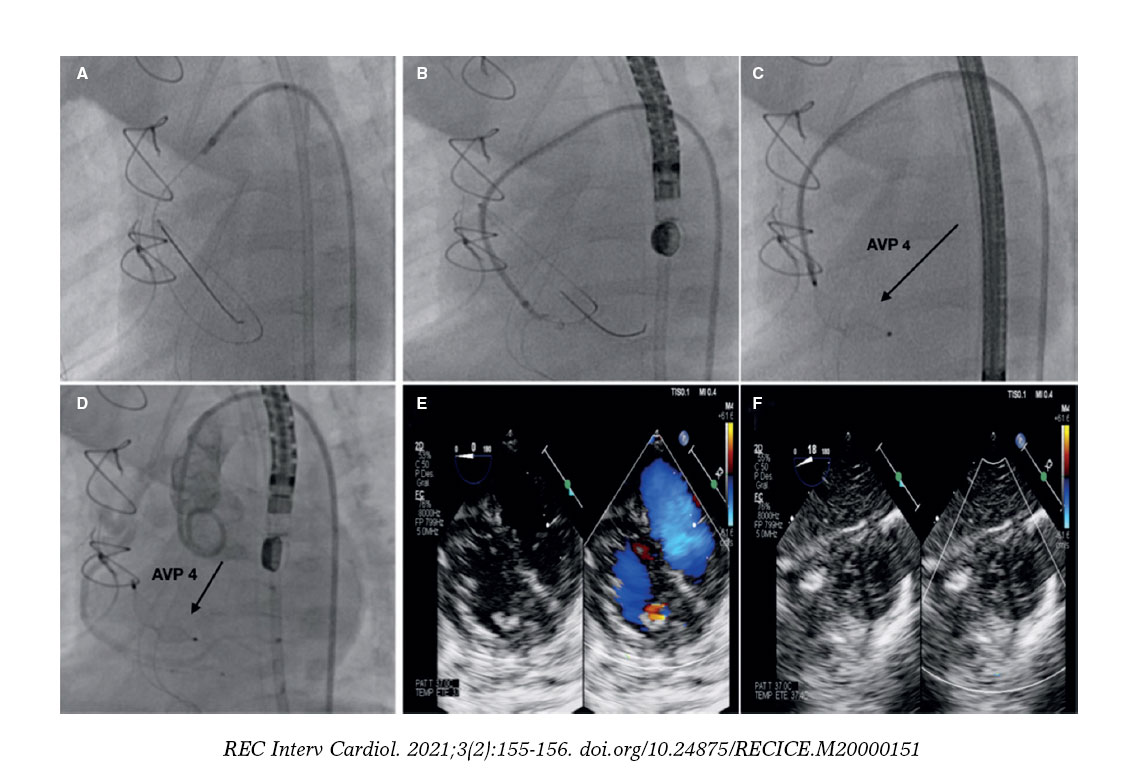
Figure 2.
Seventy-year-old male patient with an incidental finding on the transthoracic and transesophageal echocardiography of a large mass in the right atrium with abundant vascular component. Patient' informed consent was obtained for the dissemination of the case. The cardiac CT performed confirmed the finding of an arteriovenous malformation. The coronary angiography performed shows afference from the mid-right coronary artery towards the atrial mass and percutaneous closure is decided. The closure is performed by advancing a microcatheter towards the afferent branch mid-section and protecting the mid-right coronary artery through the inflation of the angioplasty balloon. Ten Hilal Coils (Cook Medical, United States) are delivered with good results and complete closure of the defect (figure 3).
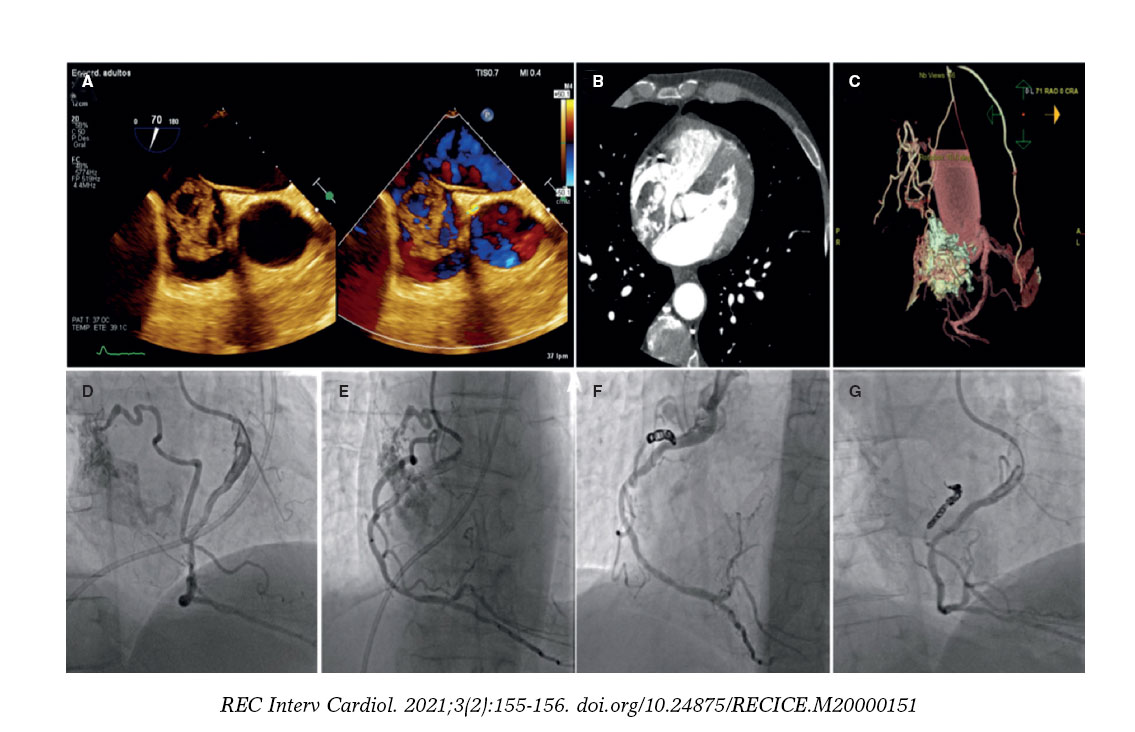
Figure 3.
FUNDING
No funding to declare.
AUTHORS' CONTRIBUTION
All authors have contributed to the elaboration, drafting and revision of the manuscript.
CONFLICTS OF INTEREST
None declared.
Corresponding author: Unidad de Cardiología Intervencionista, Plaza Cruces s/n, 48903 Baracaldo, Vizcaya, Spain.
E-mail address: luisfg82@hotmail.com (L. Fernández González).









